

Imaging of pharyngeal pathology
- PMID: 37334795
- PMCID: PMC10461270
- DOI: 10.1259/bjr.20230046
Imaging of pharyngeal pathology
Abstract
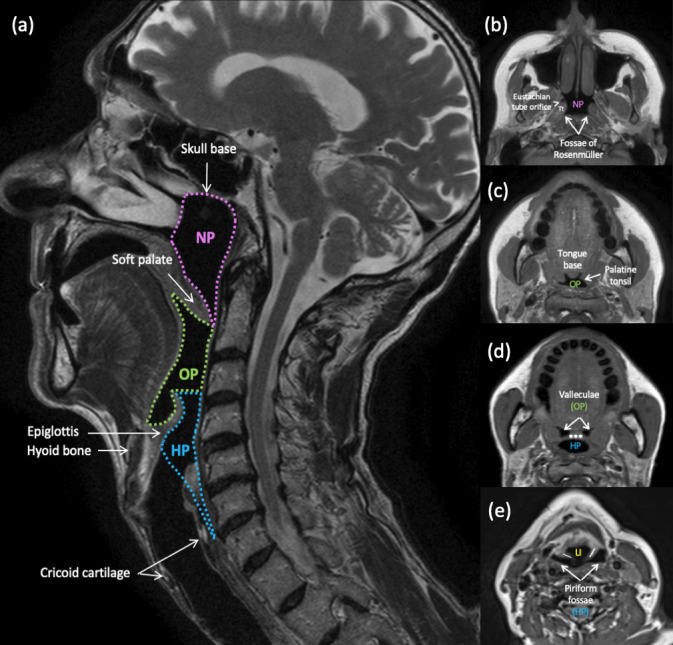
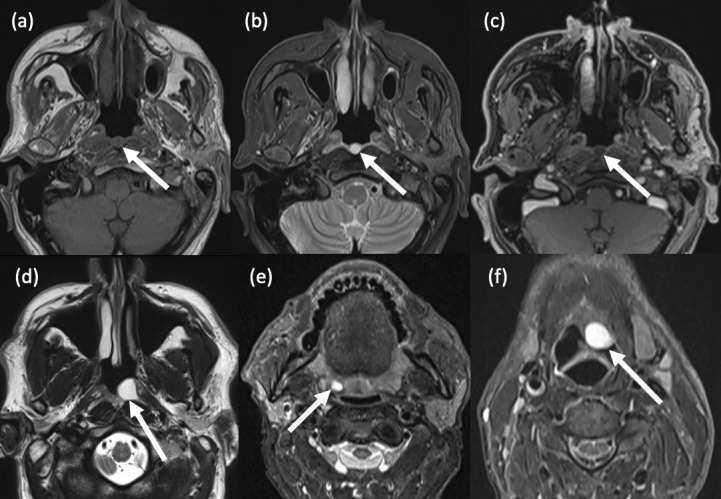
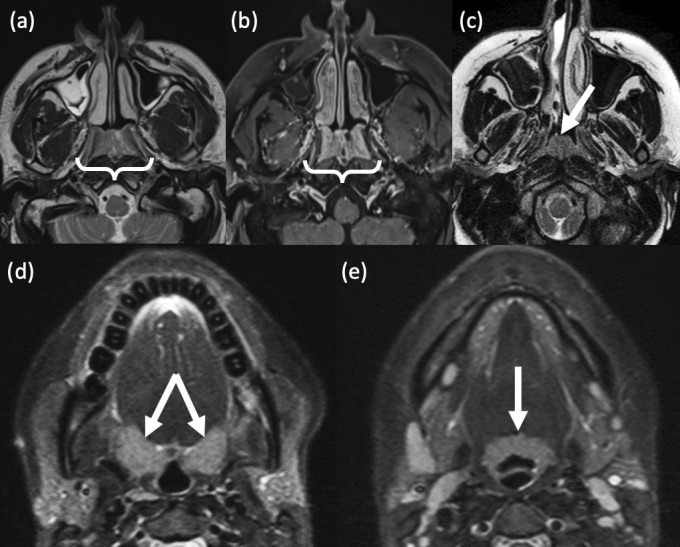
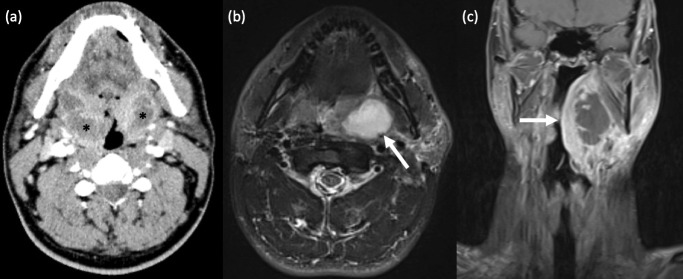
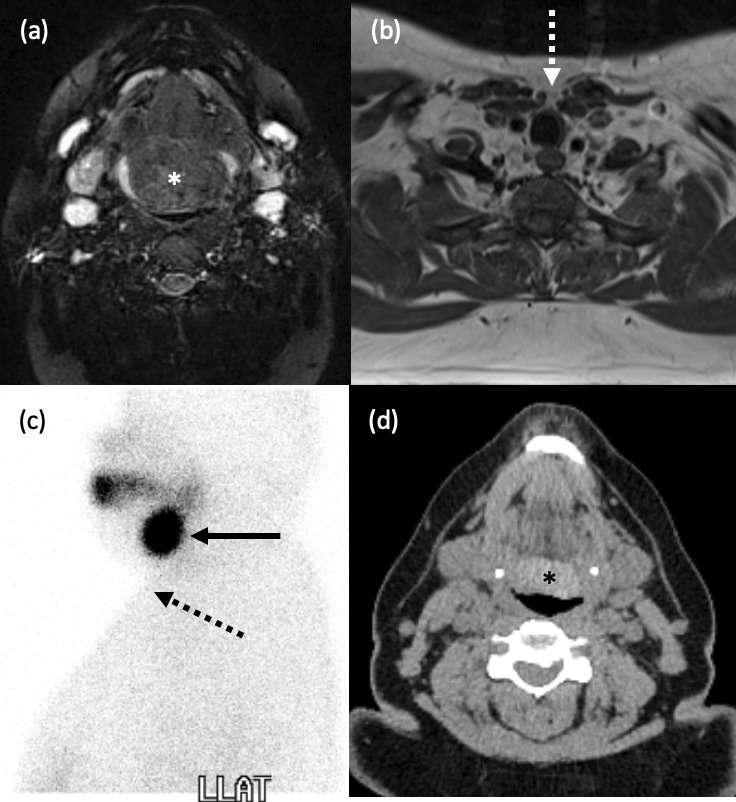
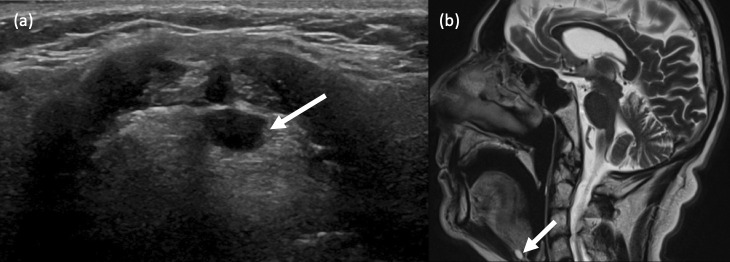
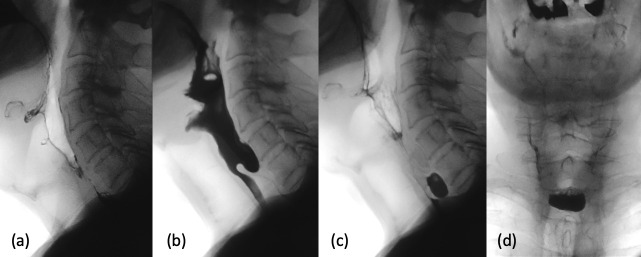
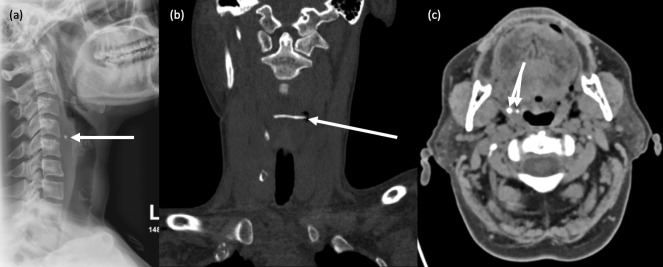
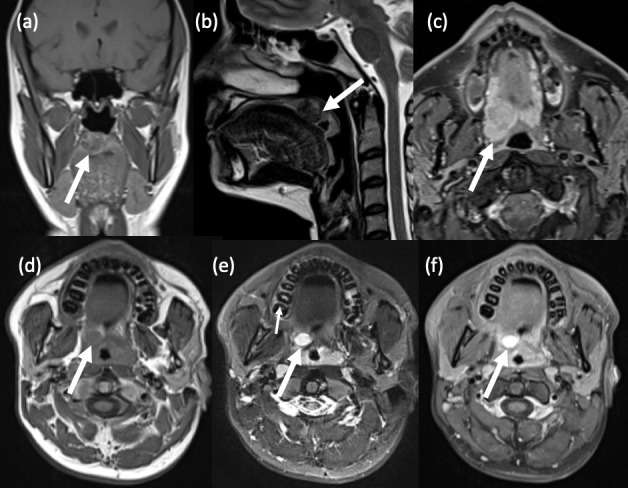
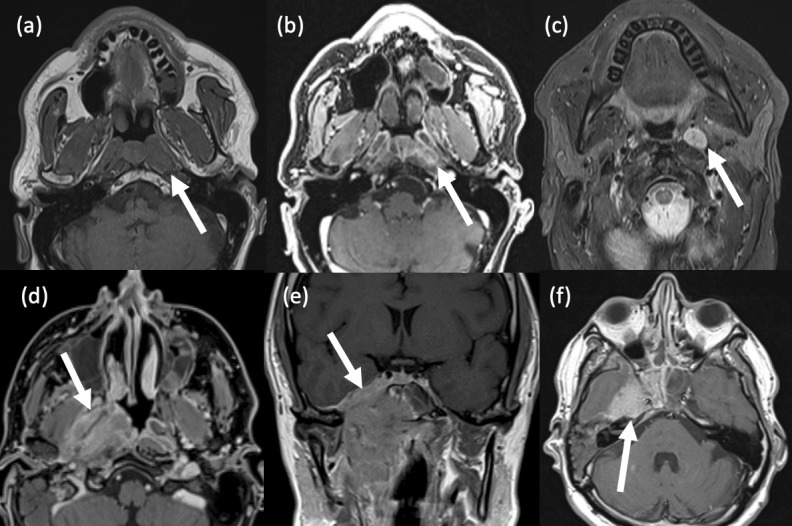
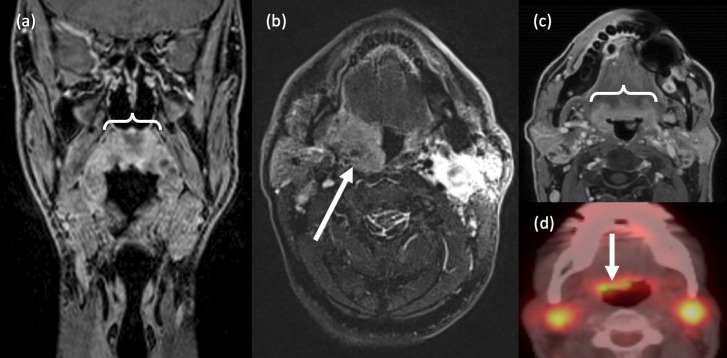
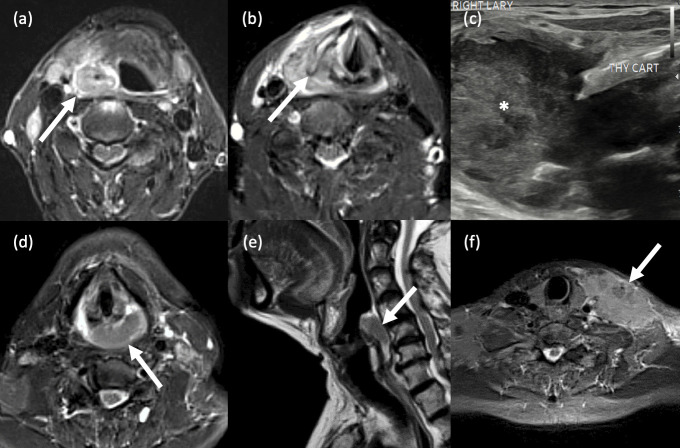
The pharynx plays a significant role in swallowing and speech, and this is reflected in both its complex anatomy and degree of physiological motility. Patients who present with pharynx-related symptoms such as sore throat, globus, dysphagia or dysphonia will usually undergo visual and nasal endoscopic examination in the first instance. Imaging is frequently required to supplement clinical assessment and this typically involves MRI and CT. However, fluoroscopy, ultrasound and radionuclide imaging are valuable in certain clinical situations. The aforementioned complexity of the pharynx and the myriad of pathologies which may arise within it often make radiological evaluation challenging. In this pictorial review, we aim to provide a brief overview of cross-sectional pharyngeal anatomy and present the radiological features of a variety of pharyngeal pathologies, both benign and malignant.
Figures

Similar articles
-
An update on pharyngeal assessment by the modified barium swallow.Abdom Radiol (NY). 2025 Jun;50(6):2414-2425. doi: 10.1007/s00261-024-04707-9. Epub 2024 Dec 8. Abdom Radiol (NY). 2025. PMID: 39648178 Free PMC article. Review.
-
Facioscapulohumeral muscular dystrophy: a radiologic and manometric study of the pharynx and esophagus.Dysphagia. 2008 Dec;23(4):341-7. doi: 10.1007/s00455-007-9141-0. Epub 2008 Feb 8. Dysphagia. 2008. PMID: 18259705
-
Radiological assessment of dysphagia in Parkinson's disease.Br J Radiol. 1991 Oct;64(766):890-3. doi: 10.1259/0007-1285-64-766-890. Br J Radiol. 1991. PMID: 1954529 Clinical Trial.
-
Detecting pharyngeal post-swallow residue by ultrasound examination: a case series.Med Ultrason. 2016 Sep;18(3):288-93. doi: 10.11152/mu.2013.2066.183.yuk. Med Ultrason. 2016. PMID: 27622403
-
Pharyngeal dysphagia: what the radiologist needs to know.Curr Probl Diagn Radiol. 2009 Jan-Feb;38(1):17-32. doi: 10.1067/j.cpradiol.2007.08.009. Curr Probl Diagn Radiol. 2009. PMID: 19041038 Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
