

Associations of Prior Head Injury With Mild Behavioral Impairment Domains
- PMID: 37335212
- PMCID: PMC10728342
- DOI: 10.1097/HTR.0000000000000880
Associations of Prior Head Injury With Mild Behavioral Impairment Domains
Abstract
Objective: This study investigated associations of prior head injury and number of prior head injuries with mild behavioral impairment (MBI) domains.
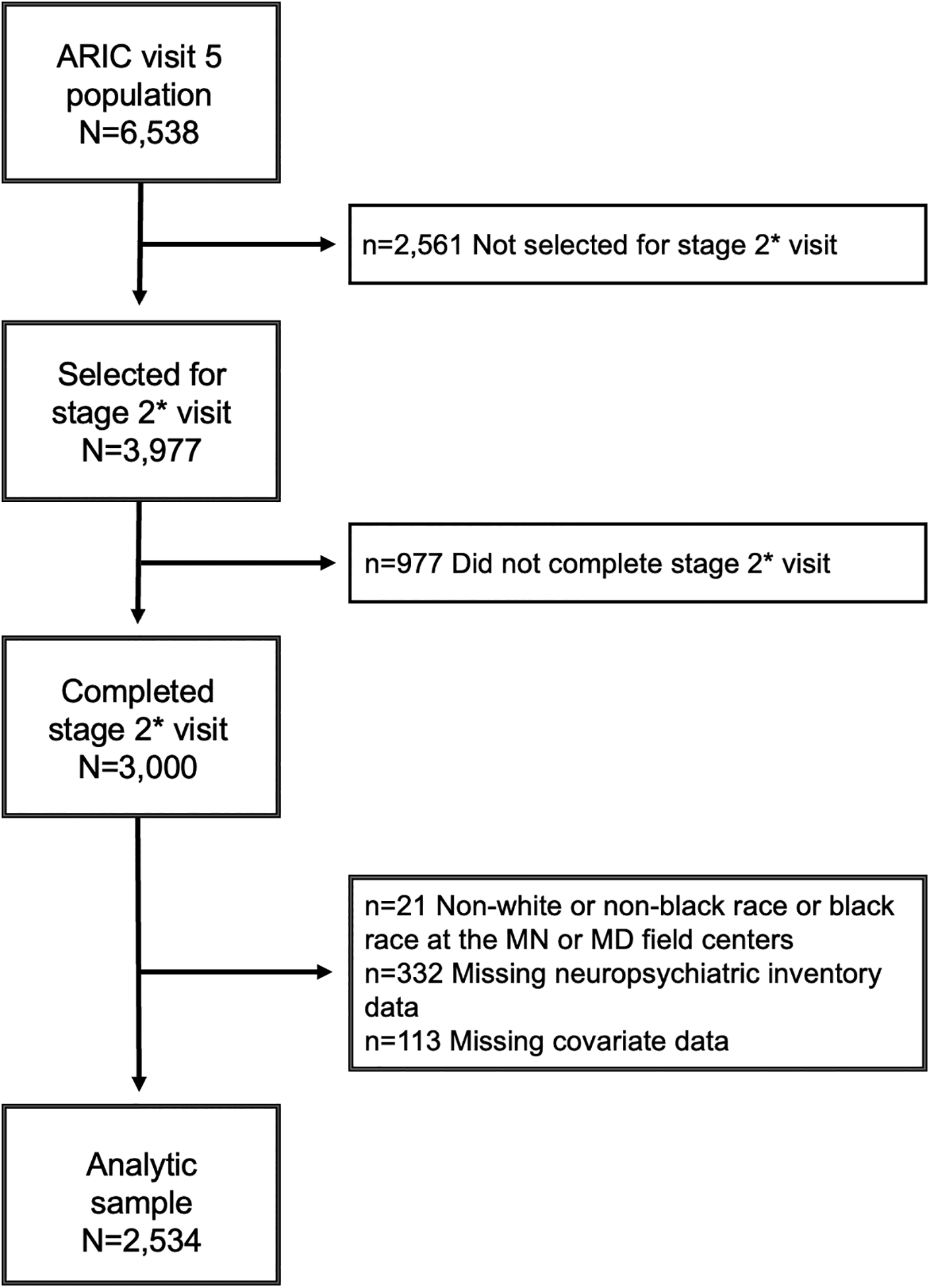
Setting: The Atherosclerosis Risk in Communities (ARIC) Study.
Participants: A total of 2534 community-dwelling older adults who took part in the ARIC Neurocognitive Study stage 2 examination were included.
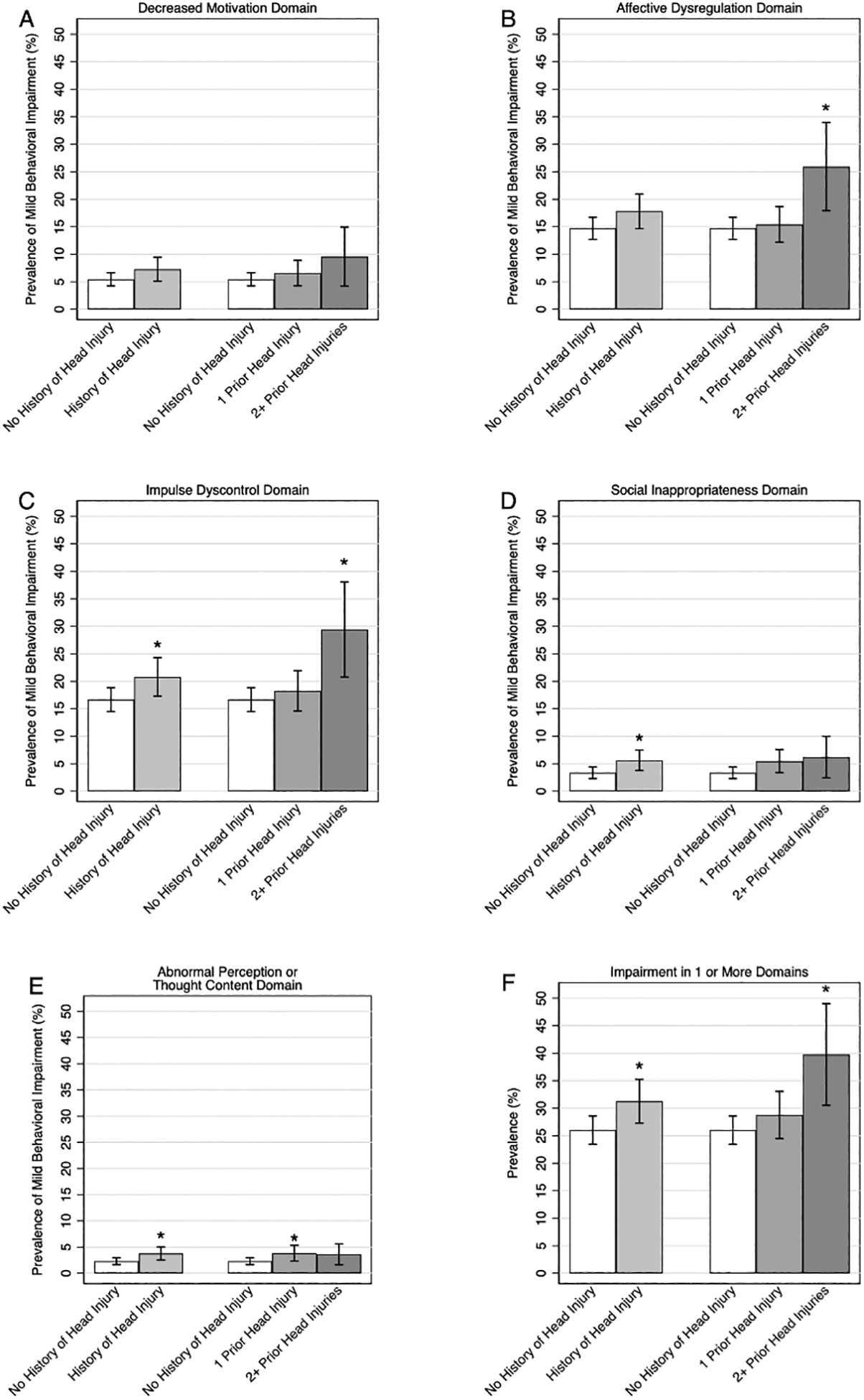
Design: This was a prospective cohort study. Head injury was defined using self-reported and International Classification of Diseases, Ninth Revision ( ICD -9) code data. MBI domains were defined using the Neuropsychiatric Inventory Questionnaire (NPI-Q) via an established algorithm mapping noncognitive neuropsychiatric symptoms to the 6 domains of decreased motivation, affective dysregulation, impulse dyscontrol, social inappropriateness, and abnormal perception/thought content.
Main measures: The primary outcome was the presence of impairment in MBI domains.
Results: Participants were a mean age of 76 years, with a median time from first head injury to NPI-Q administration of 32 years. The age-adjusted prevalence of symptoms in any 1+ MBI domains was significantly higher among individuals with versus without prior head injury (31.3% vs 26.0%, P = .027). In adjusted models, a history of 2+ head injuries, but not 1 prior head injury, was associated with increased odds of impairment in affective dysregulation and impulse dyscontrol domains, compared with no history of head injury (odds ratio [OR] = 1.83, 95% CI = 1.13-2.98, and OR = 1.74, 95% CI = 1.08-2.78, respectively). Prior head injury was not associated with symptoms in MBI domains of decreased motivation, social inappropriateness, and abnormal perception/thought content (all P > .05).
Conclusion: Prior head injury in older adults was associated with greater MBI domain symptoms, specifically affective dysregulation and impulse dyscontrol. Our results suggest that the construct of MBI can be used to systematically examine the noncognitive neuropsychiatric sequelae of head injury; further studies are needed to examine whether the systematic identification and rapid treatment of neuropsychiatric symptoms after head injury is associated with improved outcomes.
Copyright © 2024 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Ciurli P, Formisano R, Bivona U, Cantagallo A, Angelelli P. Neuropsychiatric Disorders in Persons With Severe Traumatic Brain Injury: Prevalence, Phenomenology, and Relationship With Demographic, Clinical, and Functional Features. Journal of Head Trauma Rehabilitation. 2011;26(2):116–126. doi: 10.1097/HTR.0b013e3181dedd0e - DOI - PubMed
Publication types
MeSH terms
Grants and funding
- K23 NS123340/NS/NINDS NIH HHS/United States
- U01 HL096812/HL/NHLBI NIH HHS/United States
- U01 HL096917/HL/NHLBI NIH HHS/United States
- HHSN268201700004C/HB/NHLBI NIH HHS/United States
- U01 HL096902/HL/NHLBI NIH HHS/United States
- HHSN268201700001I/HL/NHLBI NIH HHS/United States
- HHSN268201700004I/HL/NHLBI NIH HHS/United States
- U01 HL096814/HL/NHLBI NIH HHS/United States
- U01 HL096899/HL/NHLBI NIH HHS/United States
- HHSN268201700003I/HL/NHLBI NIH HHS/United States
- HHSN268201700005C/HL/NHLBI NIH HHS/United States
- HHSN268201700001C/HL/NHLBI NIH HHS/United States
- HHSN268201700002C/HB/NHLBI NIH HHS/United States
- HHSN268201700003C/HL/NHLBI NIH HHS/United States
- HHSN268201700002I/HL/NHLBI NIH HHS/United States
- HHSN268201700005I/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
