

Diagnostic challenges and forensic implications in a case of infantile fatal myocarditis
- PMID: 37335504
- PMCID: PMC10944382
- DOI: 10.1007/s12024-023-00659-6
Diagnostic challenges and forensic implications in a case of infantile fatal myocarditis
Abstract
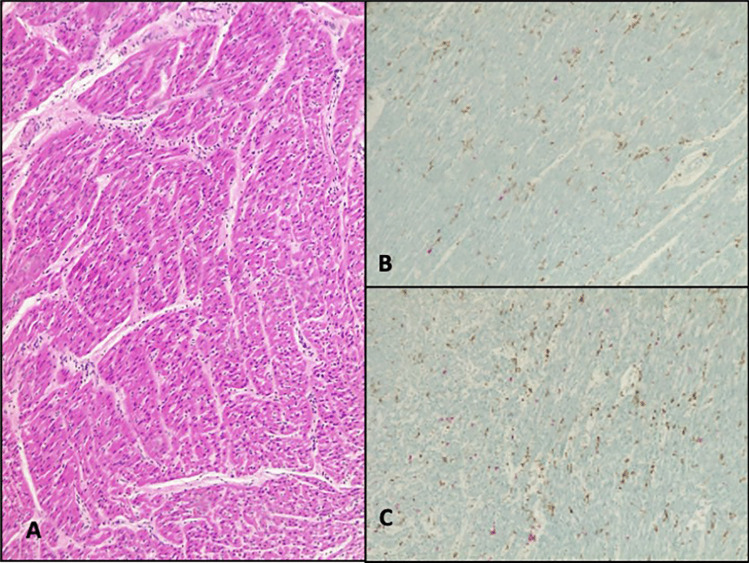
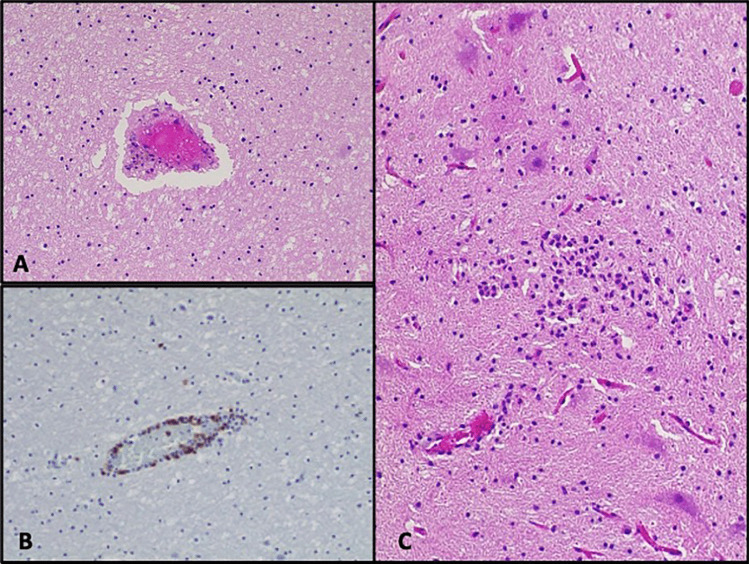
We present the case of a 23-month-old child who died less than 24 h after the onset of cardiac symptoms, despite being admitted to the hospital 72 h earlier. Autopsy revealed no significant macroscopic changes, and histologic examination revealed focal lymphocytic myocarditis with myocyte disruption, diffuse alveolar damage in the exudative phase, and generalized lymphocytic immune activation in other organs. Ante-mortem and post-mortem microbiological exams did not clearly prove a causative role of infectious agents. The peculiarity of this case was characterized by the contrast between the severe clinical features and the mild cardiac histological findings. This discrepancy, coupled with the suspicion of a viral causative role based on both ante-mortem and post-mortem microbiological examinations, presented significant challenges in reaching an etiological diagnosis. This case also confirms that the diagnosis of myocarditis in children cannot be made solely on the basis of histological cut-offs or microbiological results. Using abductive reasoning, various diagnostic hypotheses were formulated and evaluated to arrive at the final diagnosis of fatal myocarditis of viral or post-viral origin. Data from post-mortem examination are often the only source of information that is available to the experts, especially in cases of sudden infant death syndrome. In such cases, the forensic pathologists should accurately evaluate findings that may appear to indicate a different etiology, and, in the absence of clinical or radiological data, interpret post-mortem data in a logically correct manner. The autopsy is the first essential step to evaluate the cause of death and must be integrated with the results of ante- and post-mortem diagnostic tests in a holistic approach, which is crucial to allow forensic pathologists to provide an appropriate and relevant opinion.
Keywords: Autopsy; Child; Forensic medicine; Histology; Myocarditis; RT-PCR; Sudden death.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Nielsen TS, Hansen J, Nielsen LP, Baandrup UT, Banner J. The presence of enterovirus, adenovirus, and parvovirus B19 in myocardial tissue samples from autopsies: an evaluation of their frequencies in deceased individuals with myocarditis and in non-inflamed control hearts. Forensic Sci Med Pathol. 2014;10(3):344–50. doi: 10.1007/s12024-014-9570-7. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
