

Catheter-directed thrombolysis compared with systemic thrombolysis and anticoagulation in patients with intermediate- or high-risk pulmonary embolism: systematic review and network meta-analysis
- PMID: 37336568
- PMCID: PMC10281204
- DOI: 10.1503/cmaj.220960
Catheter-directed thrombolysis compared with systemic thrombolysis and anticoagulation in patients with intermediate- or high-risk pulmonary embolism: systematic review and network meta-analysis
Abstract
Background: Therapeutic options for intermediate- or high-risk pulmonary embolism (PE) include anticoagulation, systemic thrombolysis and catheter-directed thrombolysis (CDT); however, the role of CDT remains controversial. We sought to compare the efficacy and safety of CDT with other therapeutic options using network meta-analysis.
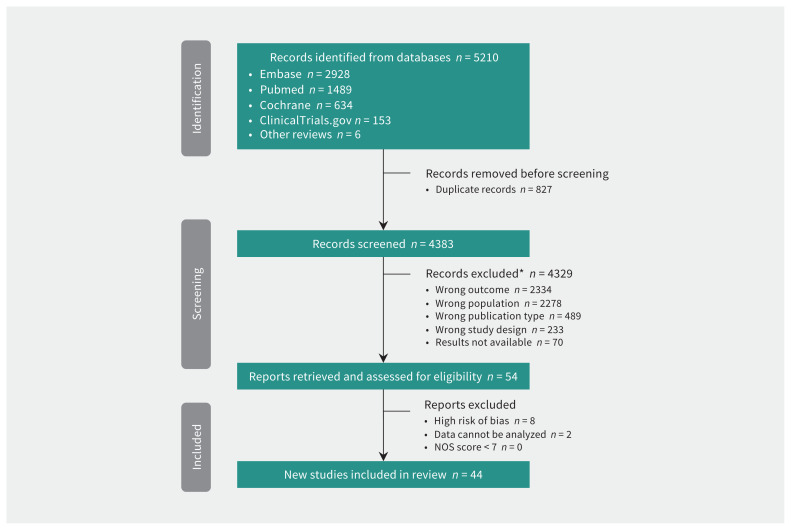
Methods: We searched PubMed (MEDLINE), Embase, ClinicalTrials.gov and Cochrane Library from inception to Oct. 18, 2022. We included randomized controlled trials and observational studies that compared therapeutic options for PE, including anticoagulation, systemic thrombolysis and CDT among patients with intermediate- or high-risk PE. The efficacy outcome was in-hospital death. Safety outcomes included major bleeding, intracerebral hemorrhage and minor bleeding.
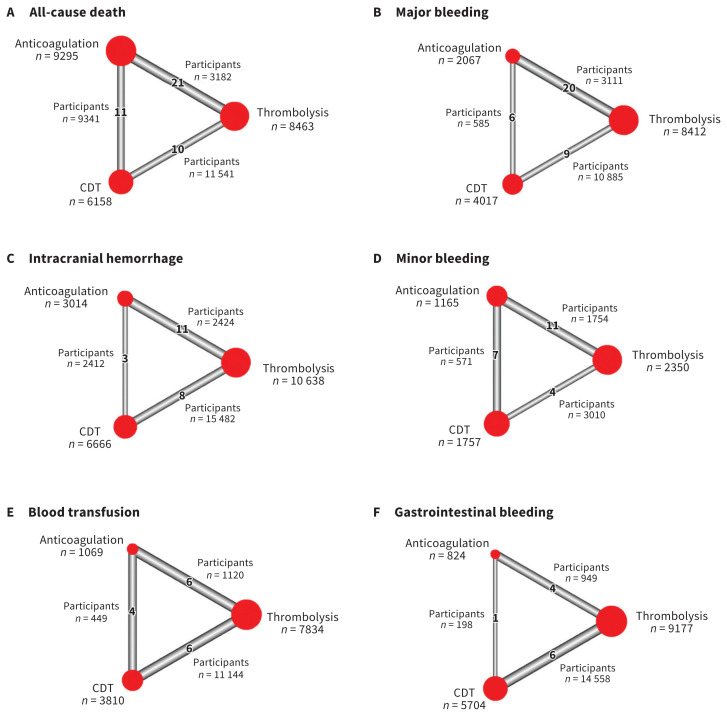
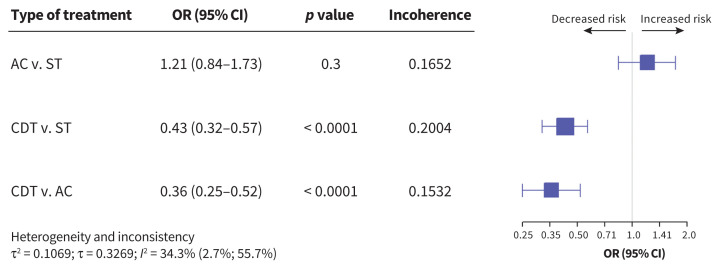
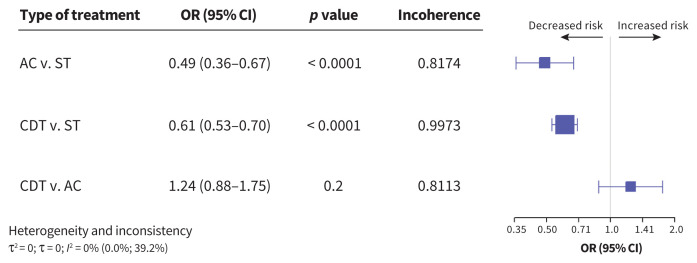
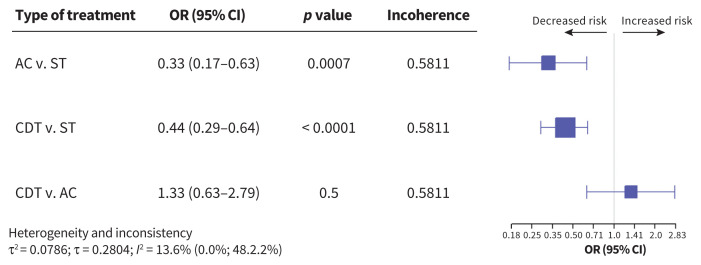
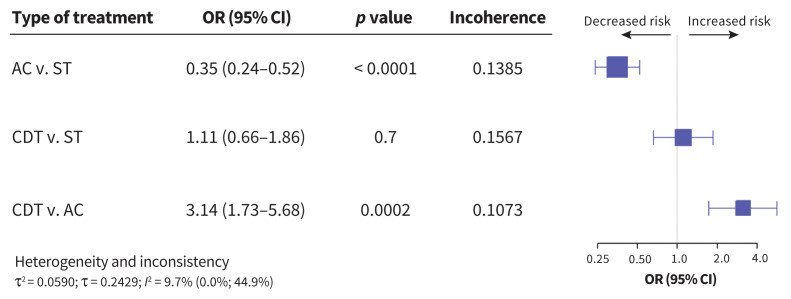
Results: We included data from 44 studies, representing 20 006 patients. Compared with systemic thrombolysis, CDT was associated with a decreased risk of death (odd ratio [OR] 0.43, 95% confidence interval [CI] 0.32-0.57), intracerebral hemorrhage (OR 0.44, 95% CI 0.29-0.64), major bleeding (OR 0.61, 95% CI 0.53-0.70) and blood transfusion (OR 0.46, 95% CI 0.28-0.77). However, no difference in minor bleeding was observed between the 2 therapeutic options (OR 1.11, 95% CI 0.66-1.87). Compared with anticoagulation, CDT was also associated with decreased risk of death (OR 0.36, 95% CI 0.25-0.52), with no increased risk of intracerebral hemorrhage (OR 1.33, 95% CI 0.63-2.79) or major bleeding (OR 1.24, 95% CI 0.88-1.75).
Interpretation: With moderate certainty of evidence, the risk of death and major bleeding complications was lower with CDT than with systemic thrombolysis. Compared with anticoagulation, CDT was associated with a probable lower risk of death and a similar risk of intracerebral hemorrhage, with moderate certainty of evidence. Although these findings are largely based on observational data, CDT may be considered as a first-line therapy in patients with intermediate- or high-risk PE.
Protocol registration: PROSPERO - CRD42020182163.
© 2023 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
In intermediate- or high-risk PE, catheter-directed thrombolysis is linked to reduced mortality vs. systemic thrombolysis or anticoagulation.Ann Intern Med. 2023 Oct;176(10):JC118. doi: 10.7326/J23-0076. Epub 2023 Oct 3. Ann Intern Med. 2023. PMID: 37782927
References
-
- Wendelboe AM, Raskob GE. Global burden of thrombosis: epidemiologic aspects. Circ Res 2016;118:1340–7. - PubMed
-
- Cohen AT, Agnelli G, Anderson FA, et al. Venous thromboembolism (VTE) in Europe – the number of VTE events and associated morbidity and mortality. Thromb Haemost 2007;98:756–64. - PubMed
-
- Konstantinides SV, Meyer G, Bueno H, et al. 2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J 2020;41:543–603. - PubMed
-
- Giri J, Sista AK, Weinberg I, et al. Interventional therapies for acute pulmonary embolism: current status and principles for the development of novel evidence: a scientific statement from the American Heart Association. Circulation 2019;140:e774–e801. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical