

Bizarre parosteal osteochondromatous proliferation: an educational review
- PMID: 37336832
- PMCID: PMC10279628
- DOI: 10.1186/s13244-023-01455-0
Bizarre parosteal osteochondromatous proliferation: an educational review
Abstract
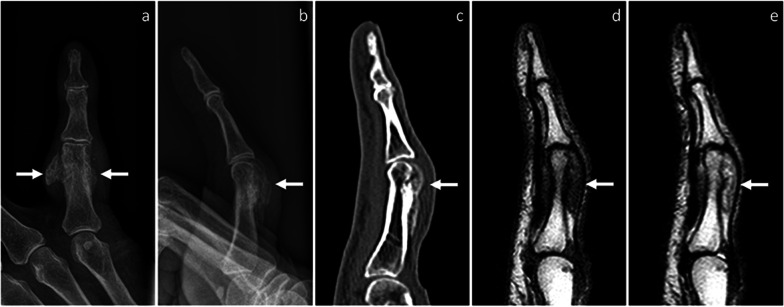
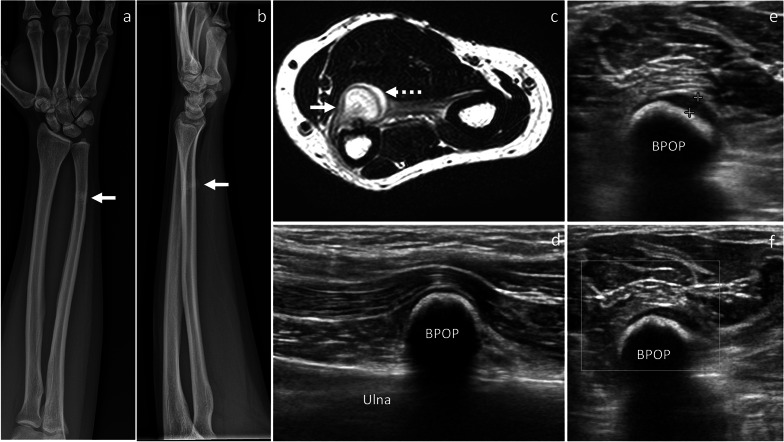
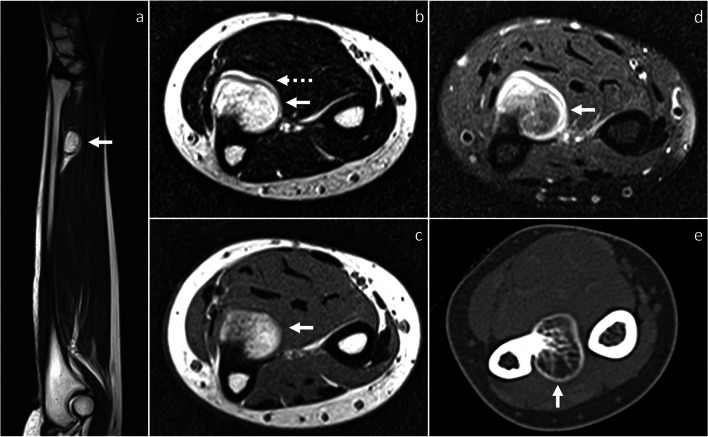
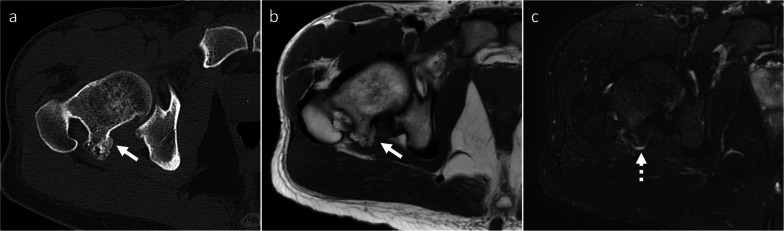
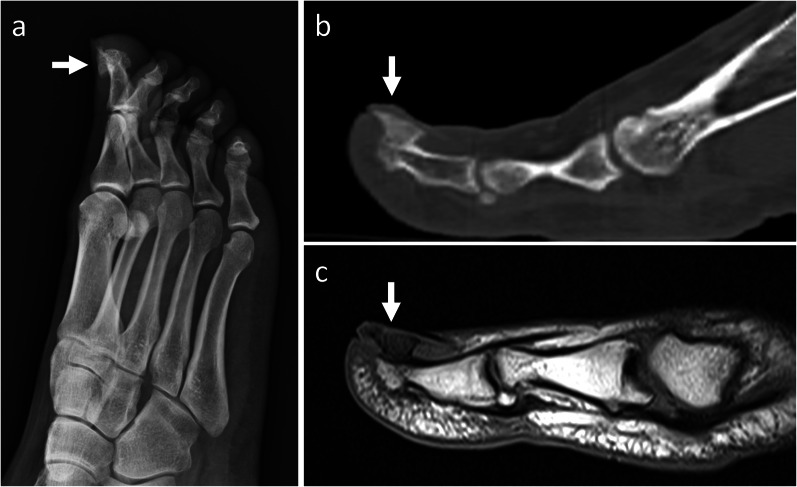
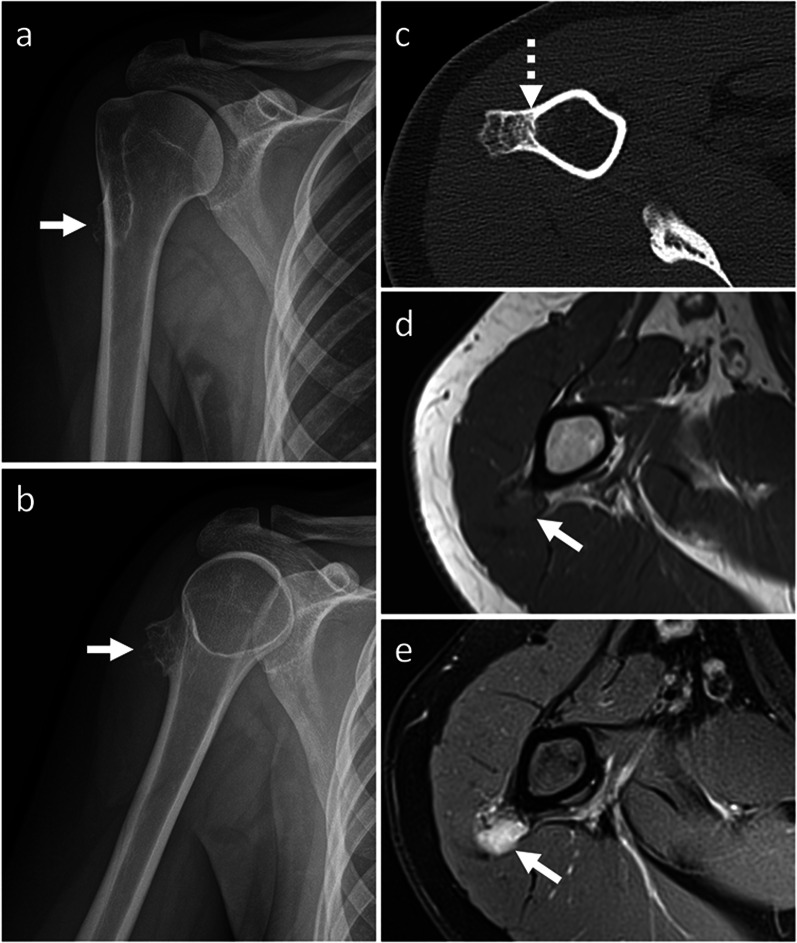
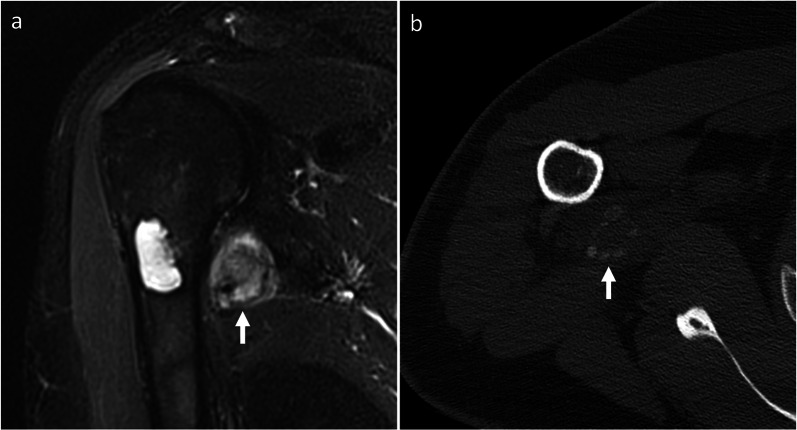
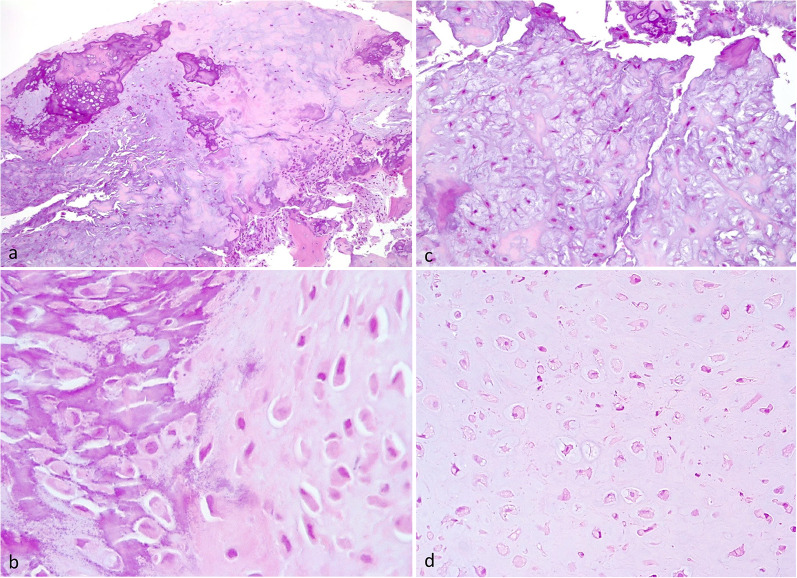
Bizarre parosteal osteochondromatous proliferation (BPOP) is a surface-based bone lesion belonging to the group of benign chondrogenic tumors. The aim of this review is to familiarize the readers with imaging features and differential diagnosis of BPOP, also addressing pathological presentation and treatment options. The peak of incidence of BPOP is in the third and fourth decades of life, although it can occur at any age. Hands are the most common location of BPOP (55%), followed by feet (15%) and long bones (25%). On imaging, BPOP appears as a well-marginated mass of heterotopic mineralization arising from the periosteal aspect of the bone. Typical features of BPOP are contiguity with the underlying bone and lack of cortico-medullary continuity, although cortical interruption and medullary involvement have been rarely reported. Histologically, BPOP is a benign bone surface lesion characterized by osteocartilaginous proliferation with disorganized admixture of cartilage with bizarre features, bone and spindle cells. Differential diagnosis includes both benign-such as florid reactive periostitis, osteochondroma, subungual exostosis, periosteal chondroma and myositis ossificans-and malignant lesions-such as periosteal chondrosarcoma and surface-based osteosarcoma. Treatment consists of surgical resection. Local recurrences are common and treated with re-excision.Critical relevance statement Bizarre parosteal osteochondromatous proliferation is a benign mineralized mass arising from the periosteal aspect of bone cortex. Multi-modality imaging characteristics, pathology features and differential diagnosis are here highlighted to familiarize the readers with this entity and offer optimal patient care.
Keywords: Bizarre parosteal osteochondromatous proliferation; Cartilaginous tumor; Nora lesion; Osteochondroma; Periostitis.
© 2023. The Author(s).
Conflict of interest statement
LM Sconfienza is member of the Insights into Imaging Advisory Editorial Board. He has not taken part in the review or selection process of this article. The remaining authors declare that they have no competing interests.
Figures




References
-
- WHO Classification of Tumours Editorial Board . WHO classification of tumours: soft tissue and bone tumours. Lyon: International Agency for Research on Cancer Press; 2020.
