

Safety and immunogenicity of a phase 1/2 randomized clinical trial of a quadrivalent, mRNA-based seasonal influenza vaccine (mRNA-1010) in healthy adults: interim analysis
- PMID: 37336877
- PMCID: PMC10279702
- DOI: 10.1038/s41467-023-39376-7
Safety and immunogenicity of a phase 1/2 randomized clinical trial of a quadrivalent, mRNA-based seasonal influenza vaccine (mRNA-1010) in healthy adults: interim analysis
Abstract
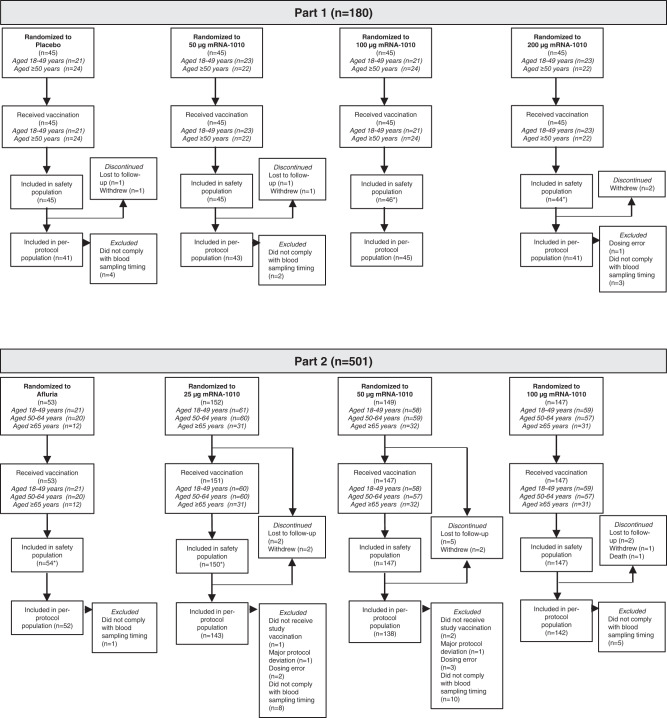
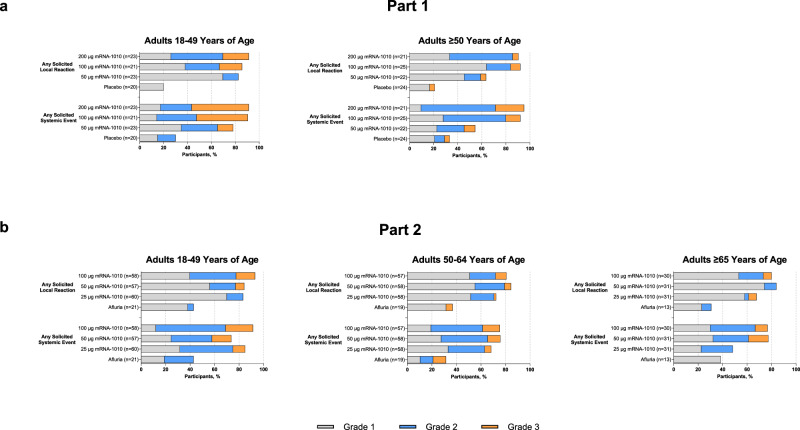
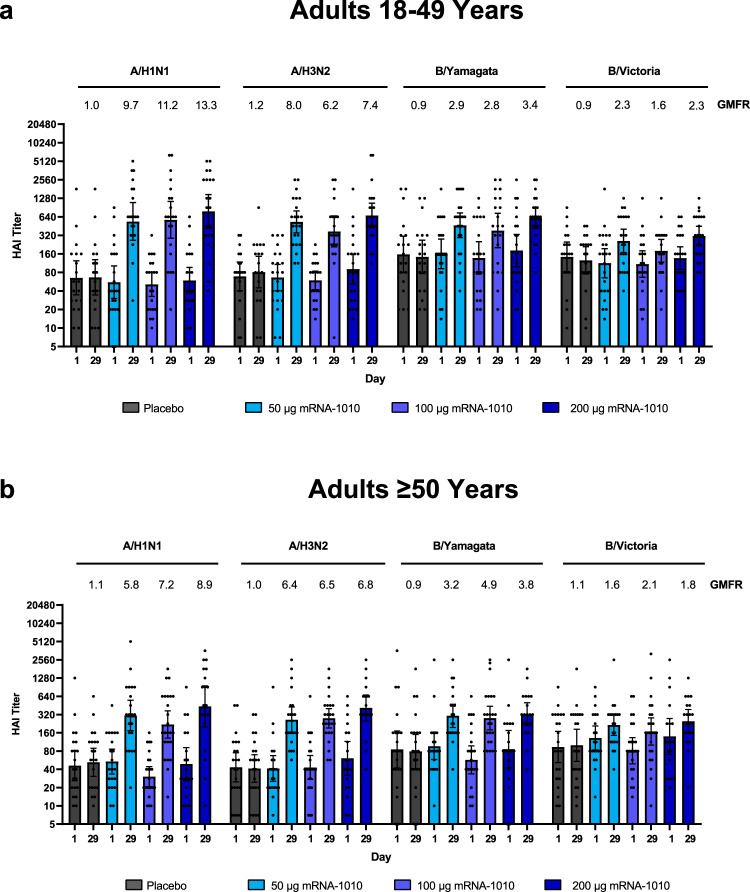
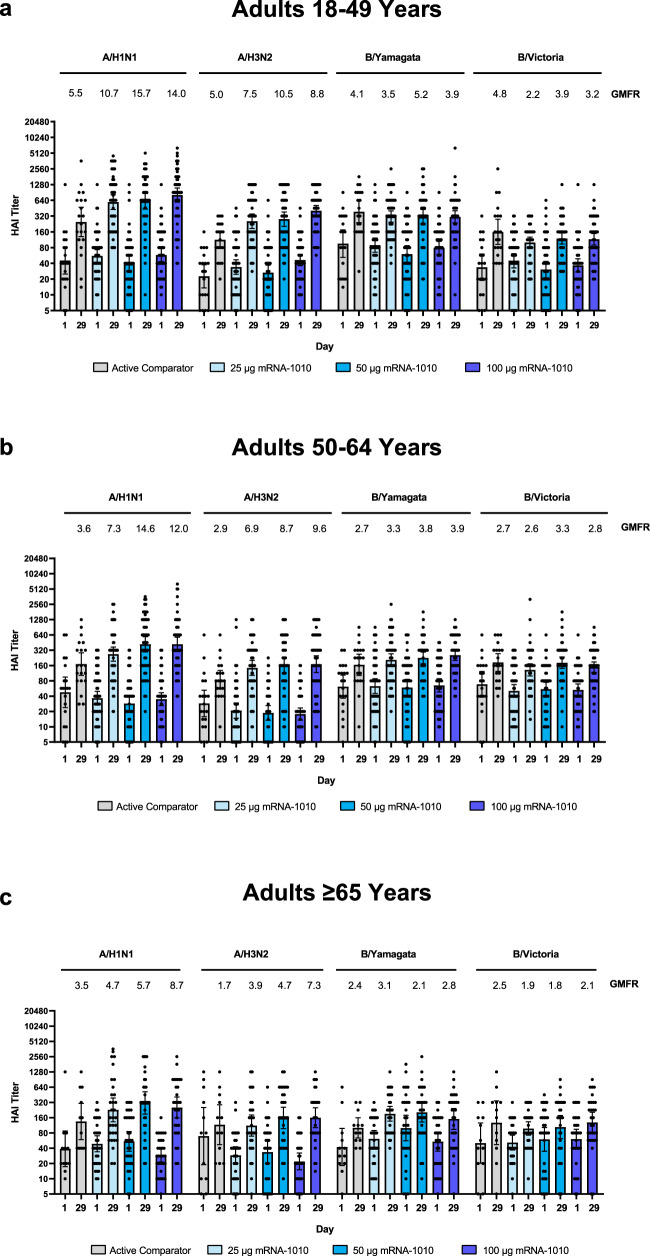
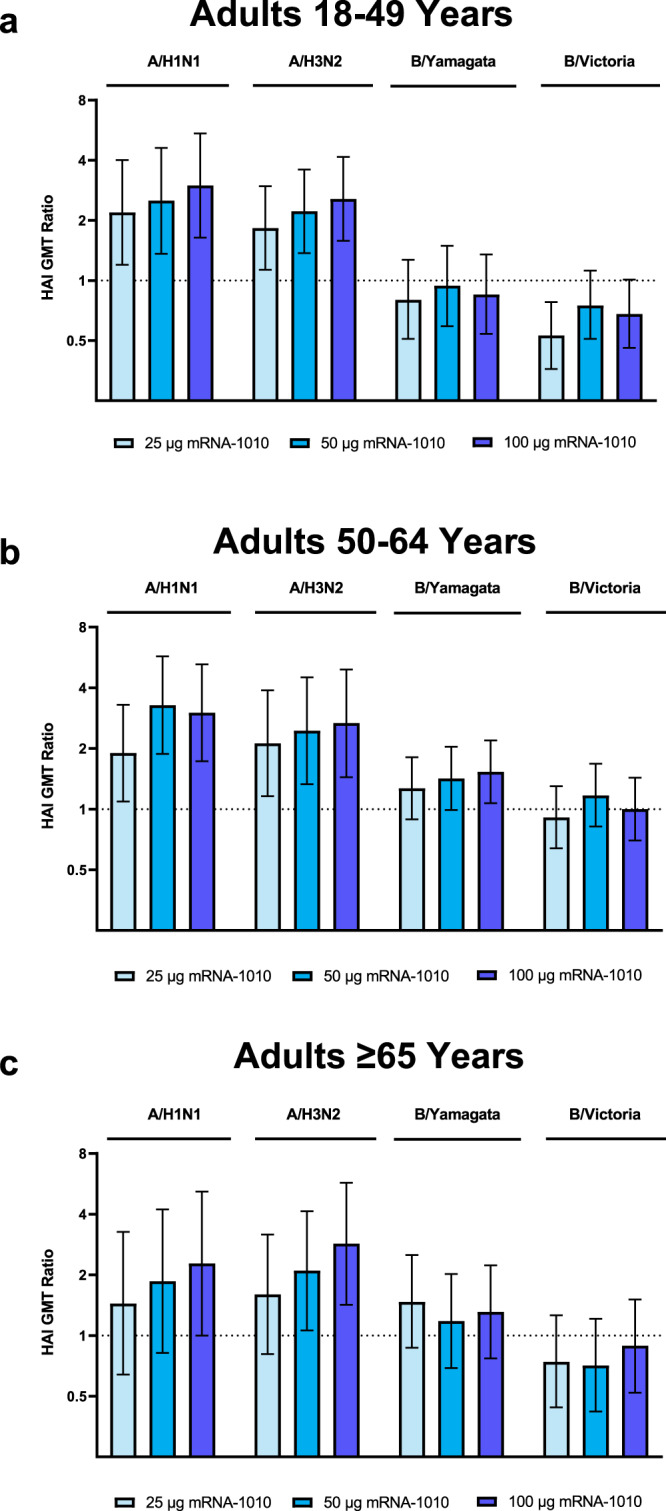
Despite vaccine availability, influenza remains a substantial global public health concern. Here, we report interim findings on the primary and secondary objectives of the safety, reactogenicity, and humoral immunogenicity of a quadrivalent messenger RNA (mRNA) vaccine against seasonal influenza, mRNA-1010, from the first 2 parts of a 3-part, first-in-human, phase 1/2 clinical trial in healthy adults aged ≥18 years (NCT04956575). In the placebo-controlled Part 1, a single dose of mRNA-1010 (50 µg, 100 µg, or 200 µg) elicited hemagglutination inhibition (HAI) titers against vaccine-matched strains. In the active-comparator-controlled Part 2, mRNA-1010 (25 µg, 50 µg, or 100 µg) elicited higher HAI titers than a standard dose, inactivated seasonal influenza vaccine for influenza A strains and comparable HAI titers for influenza B strains. No safety concerns were identified; solicited adverse reactions were dose-dependent and more frequent after receipt of mRNA-1010 than the active comparator. These interim data support continued development of mRNA-1010.
© 2023. The Author(s).
Conflict of interest statement
I.L., R.N., L.C., K.S., A.A., D.S., C.H., R.C., W.H., D.R.S., J.A., and R.P. are employees of and shareholders in Moderna, Inc. D.E. and H.S. declare no competing interests.
Figures
References
-
- World Health Organization. Vaccines against influenza: WHO position paper—May 2022. Weekly Epidemiological Record.19, 185–208 (2022).
-
- Centers for Disease Control and Prevention. Flu Vaccination Coverage, United States, 2020–21 Influenza Season. https://www.cdc.gov/flu/fluvaxview/coverage-2021estimates.htm (2021).
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
