

Advanced age is an independent prognostic factor of disease progression in high-risk prostate cancer: results in 180 patients treated with robot-assisted radical prostatectomy and extended pelvic lymph node dissection in a tertiary referral center
- PMID: 37337076
- PMCID: PMC10460358
- DOI: 10.1007/s40520-023-02466-z
Advanced age is an independent prognostic factor of disease progression in high-risk prostate cancer: results in 180 patients treated with robot-assisted radical prostatectomy and extended pelvic lymph node dissection in a tertiary referral center
Abstract
Objectives: This study aimed to assess more clinical and pathological factors associated with prostate cancer (PCa) progression in high-risk PCa patients treated primarily with robot-assisted radical prostatectomy (RARP) and extended pelvic lymph node dissection (ePLND) in a tertiary referral center.
Materials and methods: In a period ranging from January 2013 to October 2020, RARP and ePLND were performed on 180 high-risk patients at Azienda Ospedaliera Universitaria Integrata of Verona (Italy). PCa progression was defined as biochemical recurrence/persistence and/or local recurrence and/or distant metastases. Statistical methods evaluated study endpoints, including Cox's proportional hazards, Kaplan-Meyer survival curves, and binomial logistic regression models.
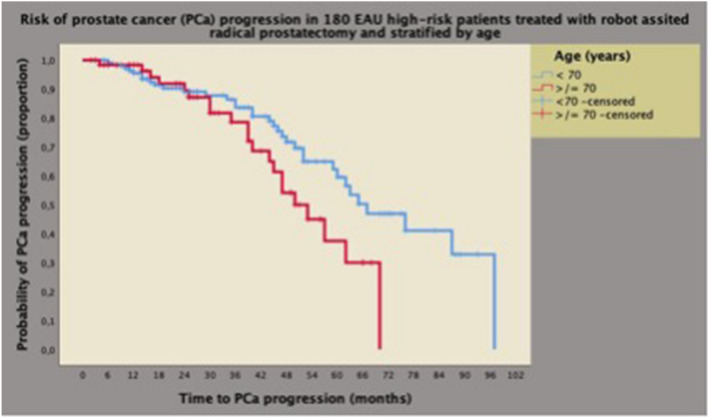
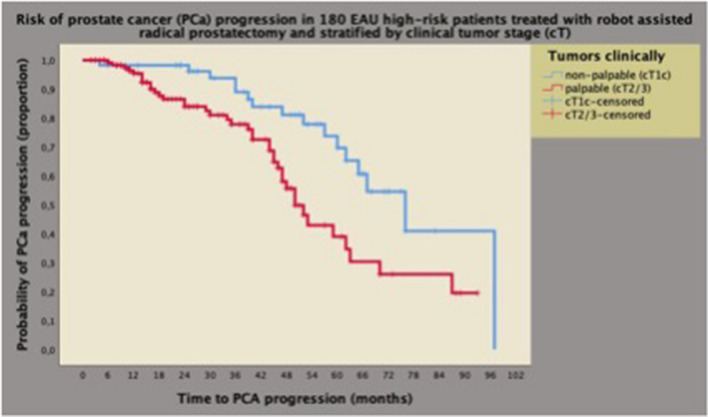
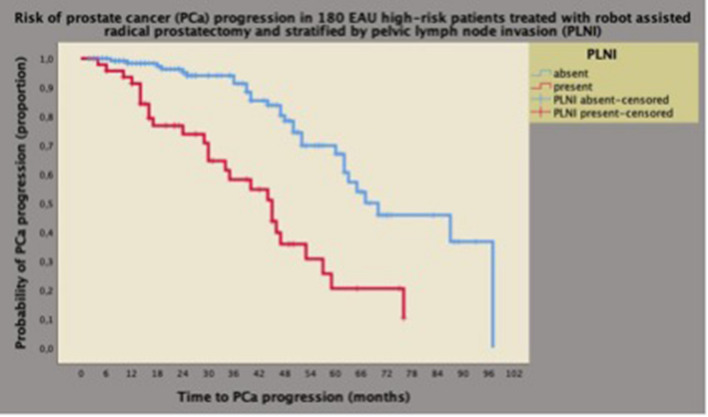
Results: The median age of included patients was 66.5 [62-71] years. Disease progression occurred in 55 patients (30.6%), who were more likely to have advanced age, palpable tumors, and unfavorable pathologic features, including high tumor grade, stage, and pelvic lymph node invasion (PLNI). On multivariate analysis, PCa progression was predicted by advanced age (≥ 70 years) (HR = 2.183; 95% CI = 1.089-4377, p = 0.028), palpable tumors (HR = 3.113; 95% CI = 1.499-6.465), p = 0.002), and PLNI (HR = 2.945; 95% CI = 1.441-6.018, p = 0.003), which were associated with clinical standard factors defining high-risk PCa. Age had a negative prognostic impact on elderly patients, who were less likely to have palpable tumors but more likely to have high-grade tumors.
Conclusions: High-risk PCa progression was independently predicted by advanced age, palpable tumors, and PLNI, which is associated with standard clinical prognostic factors. Consequently, with increasing age, the prognosis is worse in elderly patients, who represent an unfavorable age group that needs extensive counseling for appropriate and personalized management decisions.
Keywords: Adverse pathology; Intermediate-risk prostate cancer; Prognostic factors; Prognostic groups; Prostate cancer; Prostate cancer progression; Robot-assisted radical prostatectomy; Tumor upgrading; Tumor upstaging.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Mottet N, Cornford P, van den Bergh RCN, et al (2022) EAU - EANM - ESTRO - ESUR - ISUP - SIOG Guidelines on Prostate Cancer. In: European Association of Urology. https://uroweb.org/guidelines/prostate-cancer. Accessed 27 Jan 2023
-
- Schaeffer E, Srinivas S, An Y, et al (2022) Prostate Cancer, Version 1.2023, NCCN Clinical Practice Guidelines in Oncology. In: National Comprehensive Cancer Network. https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf. Accessed 27 Jan 2023 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
