

Limited wedge resection for T1 colon cancer (LIMERIC-II trial) - rationale and study protocol of a prospective multicenter clinical trial
- PMID: 37337197
- PMCID: PMC10278298
- DOI: 10.1186/s12876-023-02854-9
Limited wedge resection for T1 colon cancer (LIMERIC-II trial) - rationale and study protocol of a prospective multicenter clinical trial
Erratum in
-
Correction: Limited wedge resection for T1 colon cancer (LIMERIC-II trial) - rationale and study protocol of a prospective multicenter clinical trial.BMC Gastroenterol. 2023 Jul 27;23(1):256. doi: 10.1186/s12876-023-02905-1. BMC Gastroenterol. 2023. PMID: 37501070 Free PMC article. No abstract available.
Abstract
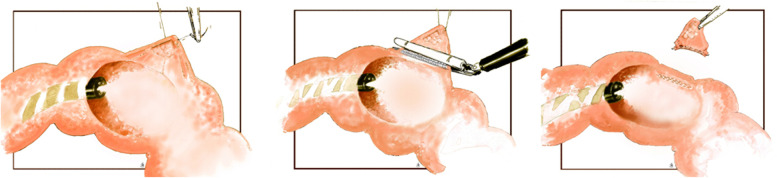
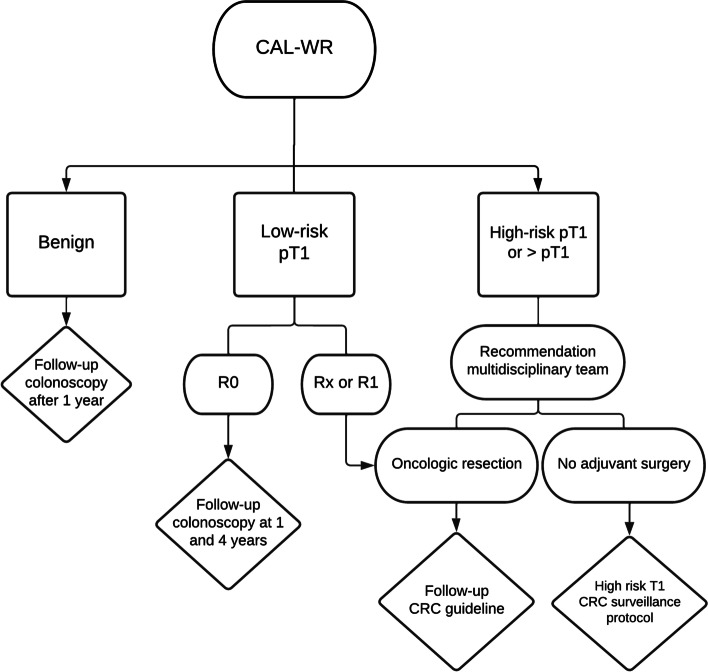
Background: The sole presence of deep submucosal invasion is shown to be associated with a limited risk of lymph node metastasis. This justifies a local excision of suspected deep submucosal invasive colon carcinomas (T1 CCs) as a first step treatment strategy. Recently Colonoscopy-Assisted Laparoscopic Wedge Resection (CAL-WR) has been shown to be able to resect pT1 CRCs with a high R0 resection rate, but the long term outcomes are lacking. The aim of this study is to evaluate the safety, effectiveness and long-term oncological outcomes of CAL-WR as primary treatment for patients with suspected superficial and also deeply-invasive T1 CCs.
Methods: In this prospective multicenter clinical trial, patients with a macroscopic and/or histologically suspected T1 CCs will receive CAL-WR as primary treatment in order to prevent unnecessary major surgery for low-risk T1 CCs. To make a CAL-WR technically feasible, the tumor may not include > 50% of the circumference and has to be localized at least 25 cm proximal from the anus. Also, there should be sufficient distance to the ileocecal valve to place a linear stapler. Before inclusion, all eligible patients will be assessed by an expert panel to confirm suspicion of T1 CC, estimate invasion depth and subsequent advise which local resection techniques are possible for removal of the lesion. The primary outcome of this study is the proportion of patients with pT1 CC that is curatively treated with CAL-WR only and in whom thus organ-preservation could be achieved. Secondary outcomes are 1) CAL-WR's technical success and R0 resection rate for T1 CC, 2) procedure-related morbidity and mortality, 3) 5-year overall and disease free survival, 4) 3-year metastasis free survival, 5) procedure-related costs and 6) impact on quality of life. A sample size of 143 patients was calculated.
Discussion: CAL-WR is a full-thickness local resection technique that could also be effective in removing pT1 colon cancer. With the lack of current endoscopic local resection techniques for > 15 mm pT1 CCs with deep submucosal invasion, CAL-WR could fill the gap between endoscopy and major oncologic surgery. The present study is the first to provide insight in the long-term oncological outcomes of CAL-WR.
Trial registration: CCMO register (ToetsingOnline), NL81497.075.22, protocol version 2.3 (October 2022).
Keywords: Colonoscopy-assisted laparoscopic wedge resection; Combined endo-laparoscopic surgery; Early-stage colorectal cancer; T1 colorectal cancer.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Ueno H, Hase K, Hashiguchi Y, Shimazaki H, Tanaka M, Miyake O, et al. Site-specific tumor grading system in colorectal cancer: multicenter pathologic review of the value of quantifying poorly differentiated clusters. Am J Surg Pathol. 2014;38(2):197–204. doi: 10.1097/PAS.0000000000000113. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
