

Is neonatal uterine bleeding responsible for early-onset endometriosis?
- PMID: 37337237
- PMCID: PMC10278367
- DOI: 10.1186/s12958-023-01099-1
Is neonatal uterine bleeding responsible for early-onset endometriosis?
Abstract
Background: It has been hypothesized that the origin of early-onset endometriosis could be from endometrial mesenchymal stem cells (eMSCs) in neonatal uterine blood (NUB). There is no information on the possible mechanistic basis linking an association between NUB/neonatal endometrium and development of early-onset endometriosis. In this study we performed a series of experiments to clarify the mechanistic link between NUB and/or neonatal endometrium and development of early-onset endometriosis.
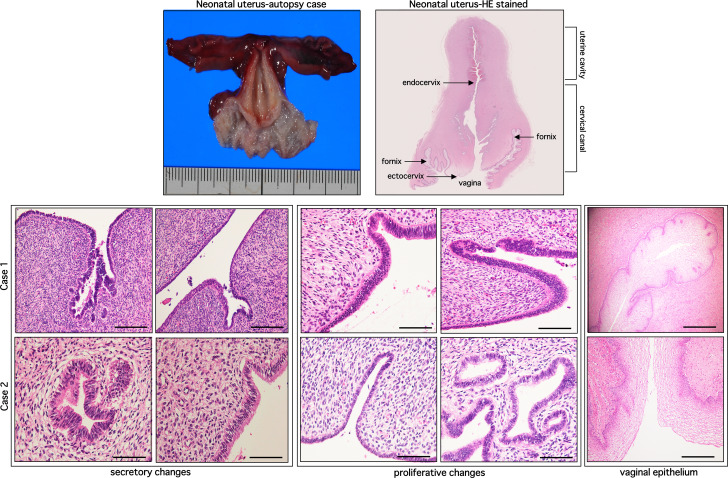
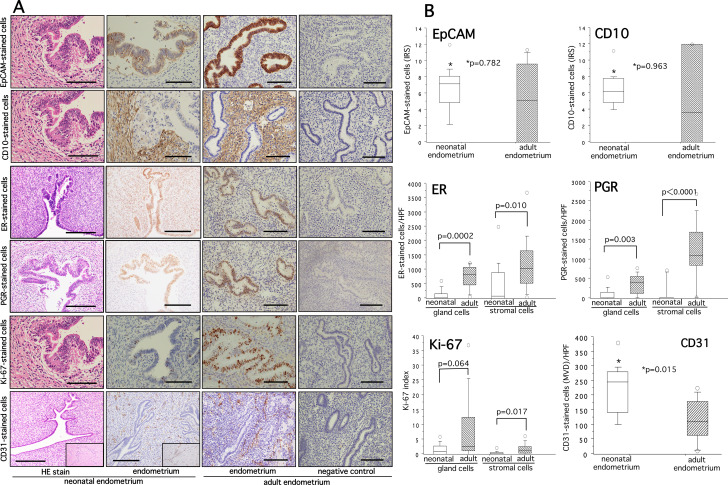
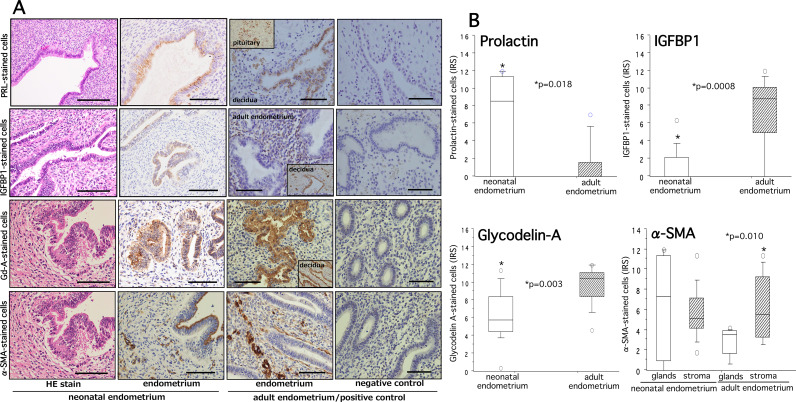
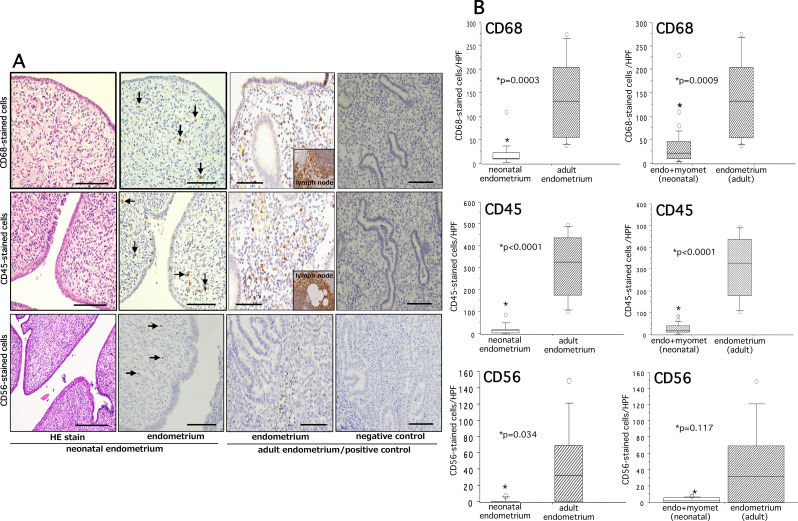
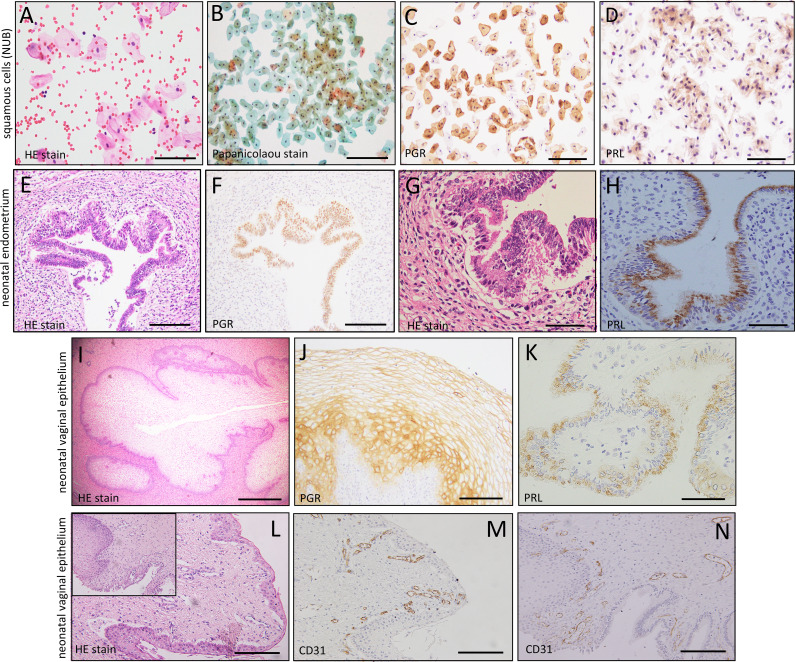
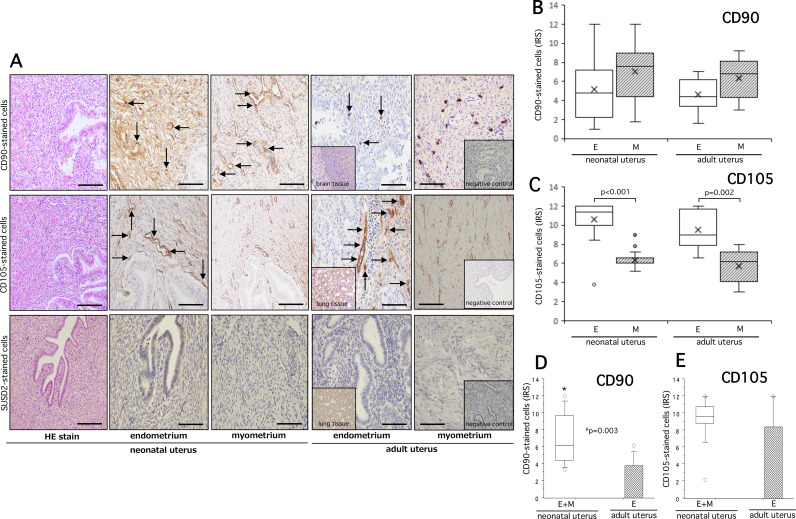
Methods: We retrospectively collected postmortem neonatal endometria (n = 15) and prospectively collected NUB (n = 18) of female babies for the analysis of different biological markers including eMSCs. Immunohistochemical analysis of neonatal endometria was performed to examine the expression patterns of ovarian steroid receptors (ER/PGR), decidualization (prolactin, IGFBP1), pre-decidualization (Glycodelin A, α-SMA), proliferation (Ki-67 index), vascularity (CD31 + cells), immunocompetent CD68+, CD45+, CD56 + cells and some putative markers of eMSCs. Cell transfer method and immunocytochemistry were used to investigate the eMSCs and/or endometrial cells in NUB.
Results: Immunohistochemical analysis of postmortem neonatal endometria revealed variable staining response to ER/PGR, decidual markers, and substantial proliferative and angiogenic activity. A moderate to strong immunoexpression of Glycodelin-A was found in both neonatal and adult endometria. The tissue infiltration of CD56+, CD45 + and CD68 + immunocompetent cells was significantly low in neonatal endometria than that in adult endometria (p = 0.0003, p < 0.0001, p = 0.034, respectively). No eMSCs or even endometrial cells were detected in NUB. However, a variable expression of some phenotypes of eMSCs (CD90/CD105) was found in neonatal endometria.
Conclusions: Based on our serial experiments we did not find any supporting evidence for the role of NUB in early-onset endometriosis. Neonatal endometria showed variable expression of ovarian steroid receptors, decidualization, and a substantial amount of proliferative and angiogenic activity. As an alternative mechanism, a significantly less tissue accumulation of immunocompetent cells in neonatal endometria may explain the survival of ER + and PGR + cells should they make entry into the pelvis and consequent development of early endometriosis with the onset of ovarian function. Future study with large sample size and application of modified technological tools is warranted to test the NUB hypothesis and to clarify their biological or clinical significance.
Trial registration: not applicable.
Keywords: Early-onset endometriosis; Immunocompetent cells; NUB hypothesis; Neonatal endometrium; Neonatal uterine blood; eMSCs.
© 2023. The Author(s).
Conflict of interest statement
All authors declare no conflict of interest.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
