

Susceptibility-guided sequential strategy versus empirical therapy for Helicobacter pylori infection: study protocol for a randomised controlled trial
- PMID: 37337241
- PMCID: PMC10278287
- DOI: 10.1186/s13063-023-07457-z
Susceptibility-guided sequential strategy versus empirical therapy for Helicobacter pylori infection: study protocol for a randomised controlled trial
Abstract
Background: New treatment strategies are required against infections caused by Helicobacter pylori, which grows increasingly resistant to antibiotics. Polymerase chain reaction-based methods for antibiotic susceptibility testing are available for detecting H. pylori-specific mutations that confer resistance to clarithromycin and levofloxacin. Several meta-analyses have compared eradication rates for susceptibility-guided versus empirical therapy for H. pylori treatment; however, all have significant limitations and high heterogeneity, and the results are contradictory. The main objective of this trial is to assess whether a sequential strategy based on molecular susceptibility testing-guided therapy for H. pylori has a better eradication rate than empirical therapy.
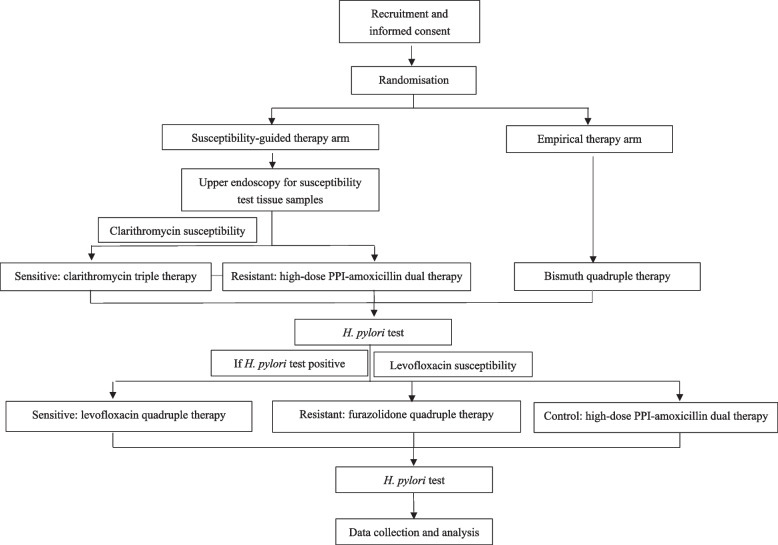
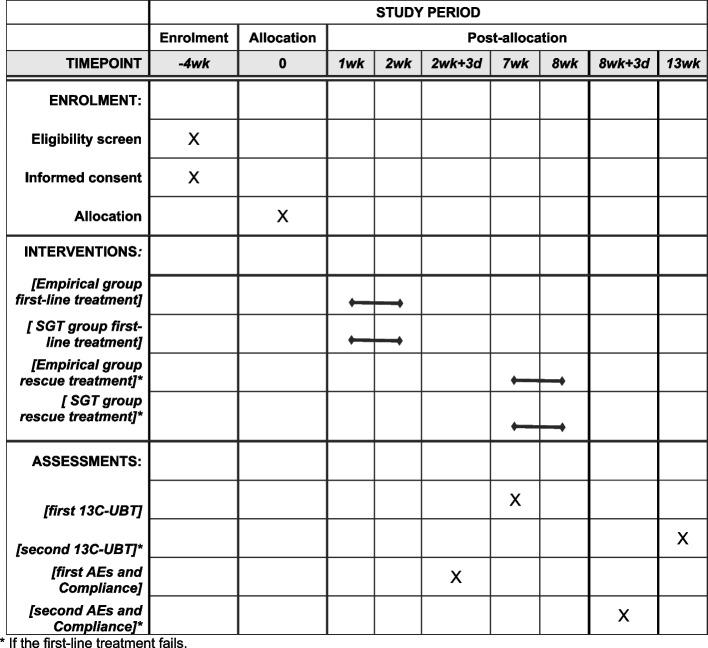
Methods: This trial is designed as a prospective, randomised, open-label, active-controlled and single-centre study. Men and women who are H. pylori-positive, naïve to treatment, and aged 18-65 years will be recruited. A total of 500 participants will be randomised to receive either empirical therapy or a susceptibility-guided sequential strategy. Bismuth quadruple therapy will be the empirical first-line therapy, and in case of failure, high-dose dual (proton-pump inhibitor + amoxicillin) treatment will be the rescue therapy. For the susceptibility-guided sequential strategy, regimen selection will be based on H. pylori susceptibility to clarithromycin (first-line) and levofloxacin (rescue). A first-line treatment of clarithromycin triple therapy will be selected for clarithromycin-sensitive strains. For clarithromycin resistance, a high-dose dual therapy will be selected. During the rescue treatment, a levofloxacin quadruple regimen will be selected for levofloxacin-sensitive strains, and a furazolidone quadruple regimen will be selected for others. The primary outcome is the first-line eradication rate in both groups, and the overall (including first and rescue therapies) H. pylori eradication rate in both groups is one of the secondary outcomes. The eradication rates of H. pylori will be analysed by intention-to-treat analysis, modified intention-to-treat analysis, and per-protocol analysis.
Discussion: This randomised controlled trial will provide objective and valid evidence about the value of polymerase chain reaction-based molecular methods for antibiotic susceptibility testing in guiding H. pylori eradication.
Trial registration: Clinicaltrials.gov NCT05549115. Released on 18 September 2022. First posted on 22 September 2022. Enrolment of the first participant on 20 September 2022. The study is retrospectively registered.
Keywords: Drug resistance; Helicobacter pylori; Microbial; Microbial sensitivity tests; Randomised controlled trial; Therapeutics.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Molecular testing-guided therapy versus susceptibility testing-guided therapy in first-line and third-line Helicobacter pylori eradication: two multicentre, open-label, randomised controlled, non-inferiority trials.Lancet Gastroenterol Hepatol. 2023 Jul;8(7):623-634. doi: 10.1016/S2468-1253(23)00097-3. Epub 2023 May 10. Lancet Gastroenterol Hepatol. 2023. PMID: 37178702 Clinical Trial.
-
Second-line levofloxacin-based quadruple therapy versus bismuth-based quadruple therapy for Helicobacter pylori eradication and long-term changes to the gut microbiota and antibiotic resistome: a multicentre, open-label, randomised controlled trial.Lancet Gastroenterol Hepatol. 2023 Mar;8(3):228-241. doi: 10.1016/S2468-1253(22)00384-3. Epub 2022 Dec 19. Lancet Gastroenterol Hepatol. 2023. PMID: 36549320 Clinical Trial.
-
Efficacy of a 2-week therapy with levofloxacin concomitant versus a levofloxacin sequential regimen for Helicobacter pylori infection in the Syrian population: a study protocol for randomized controlled trial.Trials. 2024 Jan 15;25(1):55. doi: 10.1186/s13063-024-07906-3. Trials. 2024. PMID: 38225650 Free PMC article.
-
Third-line and rescue therapy for refractory Helicobacter pylori infection: A systematic review.World J Gastroenterol. 2023 Jan 14;29(2):390-409. doi: 10.3748/wjg.v29.i2.390. World J Gastroenterol. 2023. PMID: 36687120 Free PMC article.
-
Second-line rescue treatment of Helicobacter pylori infection: Where are we now?World J Gastroenterol. 2018 Oct 28;24(40):4548-4553. doi: 10.3748/wjg.v24.i40.4548. World J Gastroenterol. 2018. PMID: 30386104 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
