

Effect of the preoperative assessment of the anteroposterior diameters of the spinal canal and dural area on the efficacy of oblique lumbar interbody fusion in patients with lumbar spinal stenosis
- PMID: 37337281
- PMCID: PMC10278331
- DOI: 10.1186/s13018-023-03913-3
Effect of the preoperative assessment of the anteroposterior diameters of the spinal canal and dural area on the efficacy of oblique lumbar interbody fusion in patients with lumbar spinal stenosis
Abstract
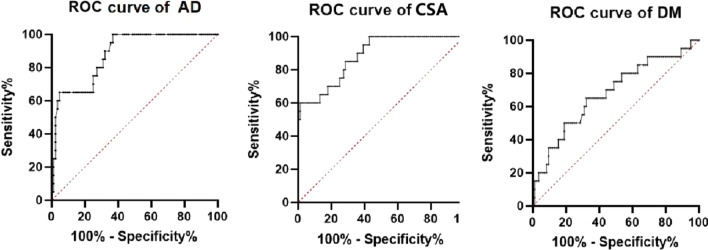
Objective: The purpose of this study was to quantify the degree of lumbar spinal stenosis by assessing the anterior and posterior vertebral canal diameter and dural area, determine the sensitivity of the anterior and posterior spinal canal diameter, dural area and dural occupying rate in predicting the postoperative efficacy of oblique lumbar interbody fusion (OLIF) for patients with single-stage lumbar spinal stenosis, and identify the corresponding indicators suggesting that OLIF surgery should not be performed.
Methods: In a retrospective analysis of patients who had previously undergone OLIF surgery in our hospital, we included a total of 104 patients with lumbar spinal stenosis who had previously undergone single-stage surgery in our hospital. Three independent observers were employed to measure the anterior and posterior diameter of the spinal canal (AD, mm), dural area (CSA, mm2), the spinal canal area (SCA, mm2), and the ratio of the dural area to the spinal canal area (DM, %) at the disc level with the most severe stenosis on MRI. According to the values of AD and CSA in preoperative MRI, patients were divided into three groups: A, B, and C (Group A: AD > 12 and 100 < CSA ≤ 130, group B: Except A and C, group C: AD ≤ 10 and CSA ≤ 75). Preoperative and postoperative clinical outcome scores (Japanese Orthopaedic Association [JOA] score, VAS score, modified Macnab standard) of 104 patients were statistically.
Results: There were significant differences in the preoperative and postoperative clinical correlation scores among the mild, moderate and severe lumbar spinal stenosis groups. The improvement rate of the post treatment JOA score, the difference between the preoperative and postoperative VAS score, and the modified Macnab standard were compared pairwise. There was no statistical significance in the improvement rate of the post treatment JOA score, the difference between the preoperative and postoperative VAS score, and the modified Macnab standard between Group A and Group B (P = 0.125, P = 0.620, P = 0.803). There were statistically significant differences between Group A and Group C and between Group B and Group C in the improvement rate of the JOA score, the difference in the pre- and postoperative VAS score, and the modified Macnab standard. The anterior and posterior vertebral canal diameter and dural area are sensitive predictors of the postoperative efficacy of OLIF surgery for single-stage lumbar spinal stenosis. Moreover, when the anterior and posterior vertebral canal diameter was less than 6.545 mm and the dural area was less than 34.43 mm2, the postoperative effect of OLIF surgery was poor.
Conclusions: All the patients with mild, moderate, and severe lumbar spinal stenosis achieved curative effects after OLIF surgery. Patients with mild and moderate lumbar spinal stenosis had better curative effects, and there was no significant difference between them, while patients with severe lumbar spinal stenosis had poor curative effects. Both the anteroposterior diameter of the spinal canal and the dural area of the spinal canal were sensitive in predicting the curative effect of OLIF surgery for single-stage lumbar spinal stenosis. When the anterior and posterior vertebral canal diameter was less than 6.545 mm and the dural area was less than 34.43 mm2, the postoperative effect of OLIF surgery was poor.
Keywords: Anteroposterior diameter; Dural area; Lumbar spinal stenosis; OLIF; Postoperative effect; Preoperative assessment.
© 2023. The Author(s).
Conflict of interest statement
All the authors declare that they have no conflict of interest.
Figures
Similar articles
-
Clinical significance of redundant nerve roots in patients with lumbar spinal stenosis undergoing oblique lumbar interbody fusion combined with percutaneous internal fixation.J Orthop Surg Res. 2023 Dec 13;18(1):958. doi: 10.1186/s13018-023-04449-2. J Orthop Surg Res. 2023. PMID: 38087350 Free PMC article.
-
[Efficacy analysis of OLIF combined with posterior percutaneous internal fixation in patients with lumbar spinal stenosis with or without redundant nerve roots].Zhongguo Gu Shang. 2024 Apr 25;37(4):345-51. doi: 10.12200/j.issn.1003-0034.20230377. Zhongguo Gu Shang. 2024. PMID: 38664203 Chinese.
-
Efficacy of OLIF combined with pedicle screw internal fixation for lumbar spinal stenosis on spinal canal changes before and after surgery.J Orthop Surg Res. 2023 Sep 25;18(1):724. doi: 10.1186/s13018-023-04209-2. J Orthop Surg Res. 2023. PMID: 37749636 Free PMC article.
-
Comparison between oblique lumbar interbody fusion and posterior lumbar interbody fusion for the treatment of lumbar degenerative diseases: a systematic review and meta-analysis.J Orthop Surg Res. 2023 Nov 10;18(1):856. doi: 10.1186/s13018-023-04312-4. J Orthop Surg Res. 2023. PMID: 37950267 Free PMC article.
-
Minimally invasive transforaminal lumbar interbody fusion versus oblique lateral interbody fusion for lumbar degenerative disease: a meta-analysis.BMC Musculoskelet Disord. 2021 Sep 18;22(1):802. doi: 10.1186/s12891-021-04687-7. BMC Musculoskelet Disord. 2021. PMID: 34537023 Free PMC article.
Cited by
-
Factors affecting outcomes of indirect decompression after oblique and lateral lumbar interbody fusions.World J Orthop. 2025 Mar 18;16(3):100772. doi: 10.5312/wjo.v16.i3.100772. eCollection 2025 Mar 18. World J Orthop. 2025. PMID: 40124722 Free PMC article.
-
LASSO Logistic Regression was Used to Analyze the Risk Factors for Cauda Equina Injury Secondary to Lumbar Spinal Stenosis and to Build a Risk Model.J Musculoskelet Neuronal Interact. 2025 Sep 1;25(3):299-306. doi: 10.22540/JMNI-25-299. J Musculoskelet Neuronal Interact. 2025. PMID: 40889195 Free PMC article.
-
Influence of decompression by laminotomy and percutaneous tansforaminal endoscopic surgery on postoperative wound healing, pain intensity, and lumbar function in elderly patients with lumbar spinal stenosis.Ann Med. 2025 Dec;57(1):2472865. doi: 10.1080/07853890.2025.2472865. Epub 2025 Mar 3. Ann Med. 2025. PMID: 40033779 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
