

The Relationship Between Hospital Capability and Mortality in Sepsis: Development of a Sepsis-Related Hospital Capability Index
- PMID: 37338282
- PMCID: PMC10615795
- DOI: 10.1097/CCM.0000000000005973
The Relationship Between Hospital Capability and Mortality in Sepsis: Development of a Sepsis-Related Hospital Capability Index
Abstract
Objectives: Regionalized sepsis care could improve sepsis outcomes by facilitating the interhospital transfer of patients to higher-capability hospitals. There are no measures of sepsis capability to guide the identification of such hospitals, although hospital case volume of sepsis has been used as a proxy. We evaluated the performance of a novel hospital sepsis-related capability (SRC) index as compared with sepsis case volume.
Design: Principal component analysis (PCA) and retrospective cohort study.
Setting: A total of 182 New York (derivation) and 274 Florida and Massachusetts (validation) nonfederal hospitals, 2018.
Patients: A total of 89,069 and 139,977 adult patients (≥ 18 yr) with sepsis were directly admitted into the derivation and validation cohort hospitals, respectively.
Interventions: None.
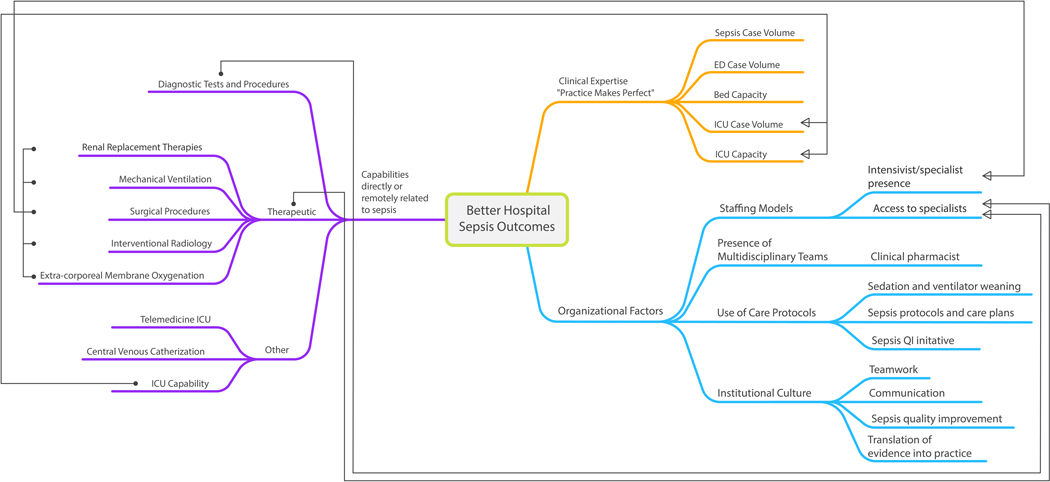
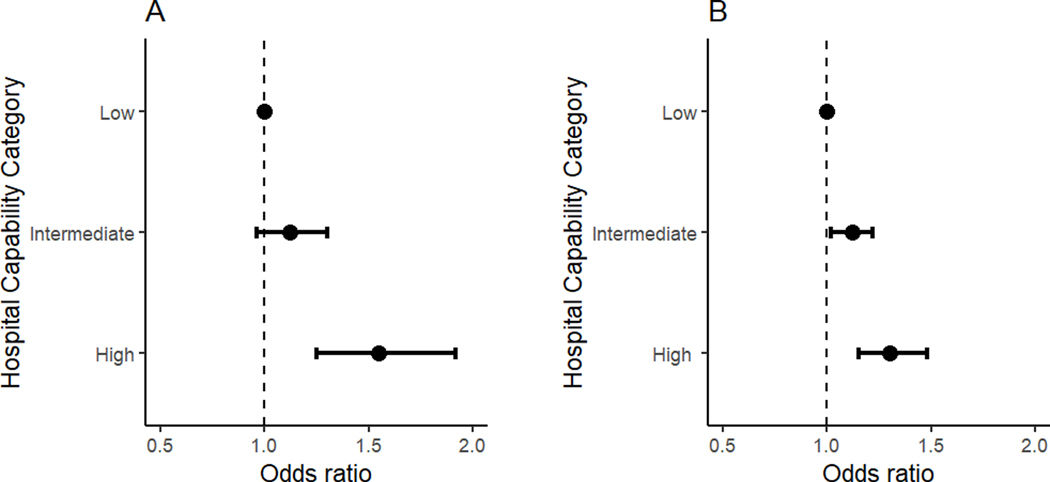
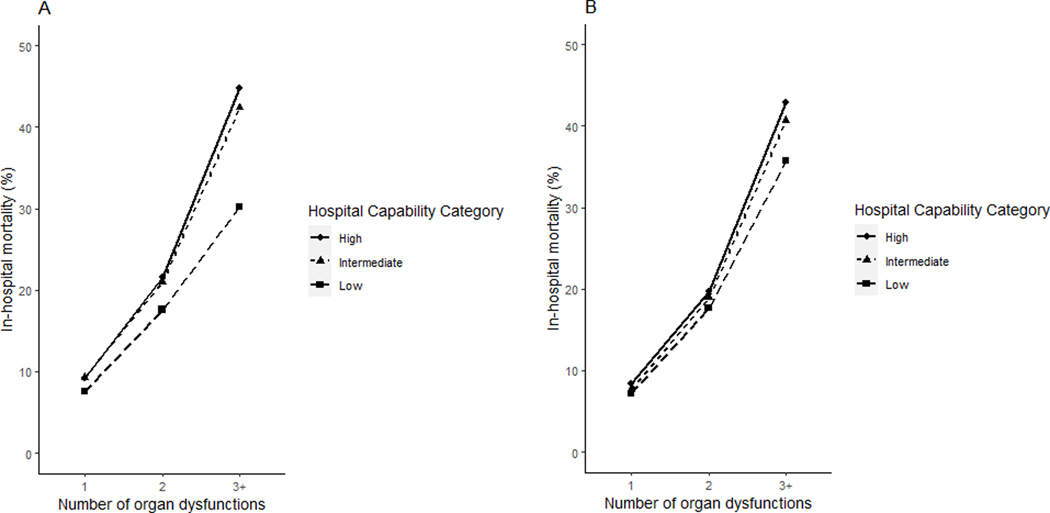
Measurements and main results: We derived SRC scores by PCA of six hospital resource use characteristics (bed capacity, annual volumes of sepsis, major diagnostic procedures, renal replacement therapy, mechanical ventilation, and major therapeutic procedures) and classified hospitals into capability score tertiles: high, intermediate, and low. High-capability hospitals were mostly urban teaching hospitals. Compared with sepsis volume, the SRC score explained more variation in hospital-level sepsis mortality in the derivation (unadjusted coefficient of determination [ R2 ]: 0.25 vs 0.12, p < 0.001 for both) and validation (0.18 vs 0.05, p < 0.001 for both) cohorts; and demonstrated stronger correlation with outward transfer rates for sepsis in the derivation (Spearman coefficient [ r ]: 0.60 vs 0.50) and validation (0.51 vs 0.45) cohorts. Compared with low-capability hospitals, patients with sepsis directly admitted into high-capability hospitals had a greater number of acute organ dysfunctions, a higher proportion of surgical hospitalizations, and higher adjusted mortality (odds ratio [OR], 1.55; 95% CI, 1.25-1.92). In stratified analysis, worse mortality associated with higher hospital capability was only evident among patients with three or more organ dysfunctions (OR, 1.88 [1.50-2.34]).
Conclusions: The SRC score has face validity for capability-based groupings of hospitals. Sepsis care may already be de facto regionalized at high-capability hospitals. Low-capability hospitals may have become more adept at treating less complicated sepsis.
Copyright © 2023 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved.
Conflict of interest statement
Dr. Ofoma’s institution received funding from the National Institute on Aging. Drs. Ofoma and Maddox received support for article research from the National Institutes of Health (NIH). Dr. Mohr’s institution received funding from Endpoint Health. Dr. Maddox’s institution received funding from the NIH; she received funding from Humana and Centene. Dr. Kollef is supported by the Barnes-Jewish Hospital Foundation. Dr. Joynt Maddox receives research support from the National Heart, Lung, and Blood Institute (R01HL143421 and R01HL164561), the National Institute of Nursing Research (U01NR020555), the National Institute on Aging (R01AG060935, R01AG063759, and R21AG065526), and from Humana. She also serves on the Health Policy Advisory Council for the Centene Corporation (St. Louis, MO). The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Unpacking Regionalization of Sepsis Care Using Hospital Capability Assessments.Crit Care Med. 2023 Nov 1;51(11):1594-1596. doi: 10.1097/CCM.0000000000005987. Epub 2023 Oct 12. Crit Care Med. 2023. PMID: 37902344 Free PMC article. No abstract available.
References
-
- Peelen L, de Keizer NF, Peek N, Scheffer GJ, van der Voort PH, de Jonge E. The influence of volume and intensive care unit organization on hospital mortality in patients admitted with severe sepsis: a retrospective multicentre cohort study. Critical care. 2007;11(2):R40. doi:10.1186/cc5727 - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
