

Incidence, prevention, risk factors, and prediction of venous thromboembolism in Chinese patients after colorectal cancer surgery: a prospective, multicenter cohort study
- PMID: 37338597
- PMCID: PMC10583908
- DOI: 10.1097/JS9.0000000000000553
Incidence, prevention, risk factors, and prediction of venous thromboembolism in Chinese patients after colorectal cancer surgery: a prospective, multicenter cohort study
Abstract
Background: Venous thromboembolism (VTE) is a common and serious complication after colorectal cancer (CRC) surgery. Few large-sample studies have reported VTE incidence and management status after CRC surgery in China. This study aimed to investigate the incidence and prevention of VTE in Chinese patients after CRC surgery, identify risk factors for developing VTE, and construct a new scoring system for clinical decision-making and care planning.
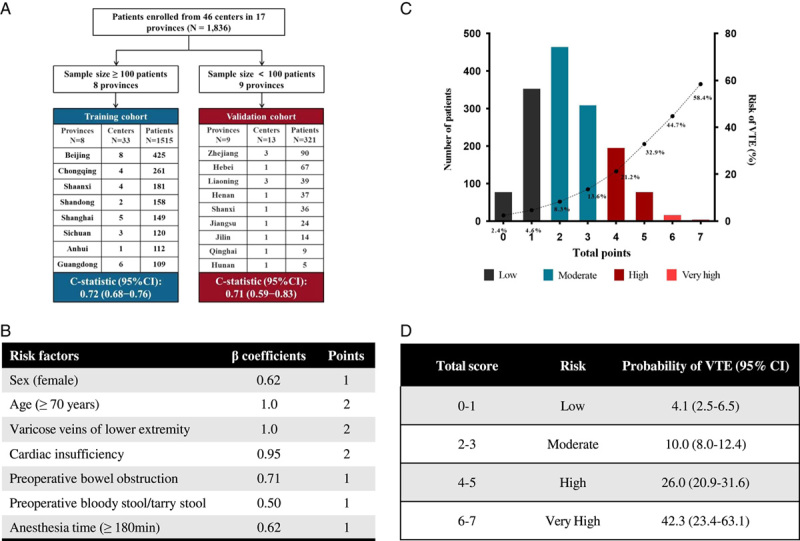
Methods: Participants were recruited from 46 centers in 17 provinces in China. Patients were followed up for 1 month postoperatively. The study period was from May 2021 to May 2022. The Caprini score risk stratification and VTE prevention and incidence were recorded. The predictors of the occurrence of VTE after surgery were identified by multivariate logistic regression analysis, and a prediction model (CRC-VTE score) was developed.
Results: A total of 1836 patients were analyzed. The postoperative Caprini scores ranged from 1 to 16 points, with a median of 6 points. Of these, 10.1% were classified as low risk (0-2 points), 7.4% as moderate risk (3-4 points), and 82.5% as high risk (≥5 points). Among these patients, 1210 (65.9%) received pharmacological prophylaxis, and 1061 (57.8%) received mechanical prophylaxis. The incidence of short-term VTE events after CRC surgery was 11.2% (95% CI 9.8-12.7), including deep venous thrombosis (DVT) (11.0%, 95% CI 9.6-12.5) and pulmonary embolism (PE) (0.2%, 95% CI 0-0.5). Multifactorial analysis showed that age (≥70 years), history of varicose veins in the lower extremities, cardiac insufficiency, female sex, preoperative bowel obstruction, preoperative bloody/tarry stool, and anesthesia time at least 180 min were independent risk factors for postoperative VTE. The CRC-VTE model was developed from these seven factors and had good VTE predictive performance ( C -statistic 0.72, 95% CI 0.68-0.76).
Conclusions: This study provided a national perspective on the incidence and prevention of VTE after CRC surgery in China. The study offers guidance for VTE prevention in patients after CRC surgery. A practical CRC-VTE risk predictive model was proposed.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

References
-
- Ay C, Pabinger I, Cohen AT. Cancer-associated venous thromboembolism: burden, mechanisms, and management. Thromb Haemost 2017;117:219–30. - PubMed
-
- Wille-Jørgensen P, Kjaergaard J, Jørgensen T, et al. Failure in prophylactic management of thromboembolic disease in colorectal surgery. Dis Colon Rectum 1988;31:384–386. - PubMed
-
- Bergqvist D. Venous thromboembolism: a review of risk and prevention in colorectal surgery patients. Dis Colon Rectum 2006;49:1620–1628. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
