

sST2 Levels Show No Association with Helicobacter pylori Infection in Asymptomatic Patients: Implications for Biomarker Research
- PMID: 37338618
- PMCID: PMC10352442
- DOI: 10.1007/s10620-023-08005-0
sST2 Levels Show No Association with Helicobacter pylori Infection in Asymptomatic Patients: Implications for Biomarker Research
Abstract
Introduction: Helicobacter pylori (H. pylori) is a prevalent stomach bacterium that can cause a range of clinical outcomes, including gastric cancer. In recent years, soluble suppression of tumorigenicity-2 (sST2) has gained attention as a biomarker associated with various diseases, such as gastric cancer. The purpose of this study was to explore the possible connection between H. pylori infection and sST2 levels in patients who do not exhibit symptoms.
Methods: A total of 694 patients from the Salzburg Colon Cancer Prevention Initiative (Sakkopi) were included in the study. The prevalence of H. pylori infection was determined by histology, and sST2 levels were measured in serum samples. Clinical and laboratory parameters, such as age, sex, BMI, smoking status, hypertension, and metabolic syndrome, were also collected.
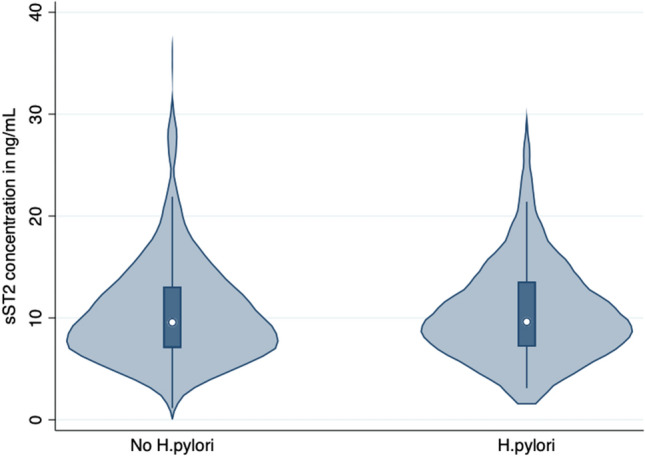
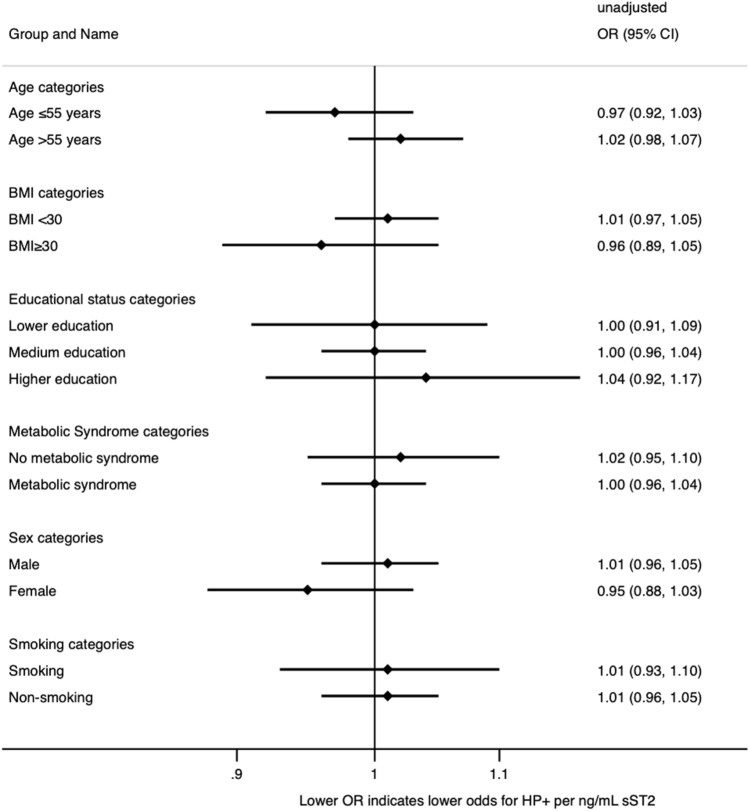
Results: The median sST2 concentration was similar between patients with (9.62; 7.18-13.44 ng/mL; p = 0.66) and without (9.67; 7.08-13.06 ng/mL) H. pylori. Logistic regression analysis did not show any association (OR 1.00; 95%CI 0.97-1.04; p = 0.93) between sST2 levels and H. pylori infection, which remained so (aOR 0.99; 95%CI 0.95-1.03; p = 0.60) after adjustment for age, sex, educational status, and metabolic syndrome. In addition, sensitivity analyses stratified by age, sex, BMI, smoking status, educational status, and the concomitant diagnosis of metabolic syndrome could not show any association between sST2 levels and H. pylori infection.
Conclusion: The results indicate that sST2 may not serve as a valuable biomarker in the diagnosis and treatment of H. pylori infection. Our findings are of relevance for further research investigating sST2, as we could not find an influence of asymptomatic H. pylori infection on sST2 concentration. WHAT IS ALREADY KNOWN?: Soluble suppression of tumorigenicity-2 (sST2) has gained attention as a biomarker associated with various diseases, such as gastric cancer. WHAT IS NEW IN THIS STUDY?: The median sST2 concentration was similar between patients with (9.62; 7.18-13.44 ng/mL; p = 0.66) and without (9.67; 7.08-13.06 ng/mL) H. pylori. WHAT ARE THE FUTURE CLINICAL AND RESEARCH IMPLICATIONS OF THE STUDY FINDINGS?: The results indicate that sST2 may not serve as a valuable biomarker in the diagnosis and treatment of H. pylori infection.
Keywords: Biomarker; Cancer; H. pylori; Soluble suppression of tumorigenicity-2; sST2.
© 2023. The Author(s).
Conflict of interest statement
CD is part of the scientific advisory board of SPAR Austria.
Figures
Similar articles
-
Assessing the association between H. pylori infection and educational status: implications for screening strategies?Minerva Gastroenterol (Torino). 2024 Jun;70(2):171-176. doi: 10.23736/S2724-5985.23.03404-6. Epub 2023 Jun 13. Minerva Gastroenterol (Torino). 2024. PMID: 37310371
-
[Helicobacter pylori CagA(+) infection in gastric cancer patients].Pol Merkur Lekarski. 2002 Sep;13(75):216-20. Pol Merkur Lekarski. 2002. PMID: 12474574 Polish.
-
Risk Factors and Incidence of Gastric Cancer After Detection of Helicobacter pylori Infection: A Large Cohort Study.Gastroenterology. 2020 Feb;158(3):527-536.e7. doi: 10.1053/j.gastro.2019.10.019. Epub 2019 Oct 22. Gastroenterology. 2020. PMID: 31654635 Free PMC article.
-
Biomarkers of Helicobacter pylori-associated gastric cancer.Gut Microbes. 2013 Nov-Dec;4(6):532-40. doi: 10.4161/gmic.25720. Epub 2013 Jul 12. Gut Microbes. 2013. PMID: 23851317 Free PMC article. Review.
-
Diagnosis of Helicobacter pylori Infection.Asian Pac J Cancer Prev. 2016;17(4):1631-5. doi: 10.7314/apjcp.2016.17.4.1631. Asian Pac J Cancer Prev. 2016. PMID: 27221831 Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
