

Review
doi: 10.1007/978-3-031-26220-3_13.
Epub 2023 Jun 21.
Clinical Implications of Dystonia as a Neural Network Disorder
Affiliations
- PMID: 37338705
- PMCID: PMC10319344
- DOI: 10.1007/978-3-031-26220-3_13
Item in Clipboard
Review
Clinical Implications of Dystonia as a Neural Network Disorder
Adv Neurobiol.
2023.
Abstract
Isolated dystonia is a neurological disorder of diverse etiology, multifactorial pathophysiology, and wide spectrum of clinical presentations. We review the recent neuroimaging advances that led to the conceptualization of dystonia as a neural network disorder and discuss how current knowledge is shaping the identification of biomarkers of dystonia and the development of novel pharmacological therapies.
Keywords: Connectome; Functional connectivity; Network disorder; Neurotransmission; Structural networks.
© 2023. Springer Nature Switzerland AG.
Figures
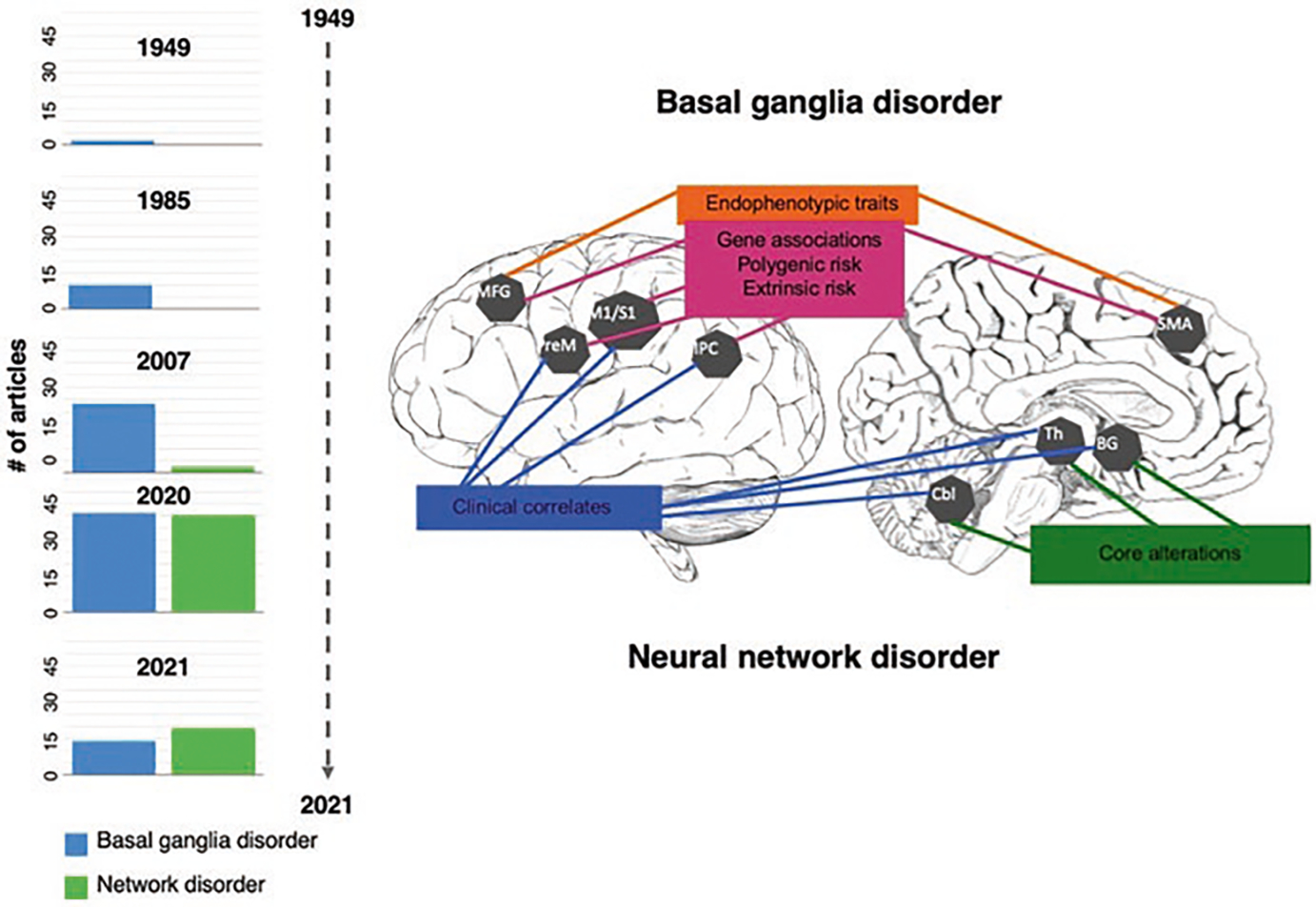
Imaging signatures of dystonia and timeline of the basal ganglia vs. neural network disorder evolution. Schematic representation of the main regions of abnormal brain function, structure, and metabolism in dystonia and their associations with genes, endophenotypic traits, clinical features, and extrinsic/environmental risk (Adapted from Simonyan et al. [101]). The bar graphs of the timeline show how the view of the pathophysiology of dystonia changed over the years from a basal ganglia to a neural network disorder. Based on the literature search in PubMed, bars graphs show the number of articles published across the years considering dystonia a basal ganglia disorder, or a network disorder. The terms used for the search included: “idiopathic dystonia OR primary dystonia OR isolated dystonia AND brain AND basal ganglia disorder” and “idiopathic dystonia OR primary dystonia OR isolated dystonia AND brain AND network disorder.” Abbreviations: MGF middle frontal gyrus, PreM premotor cortex, M1/S1 primary sensorimotor cortex, IPC inferior parietal cortex, SMA supplementary motor area, BG basal ganglia, Th thalamus, Cbl cerebellum
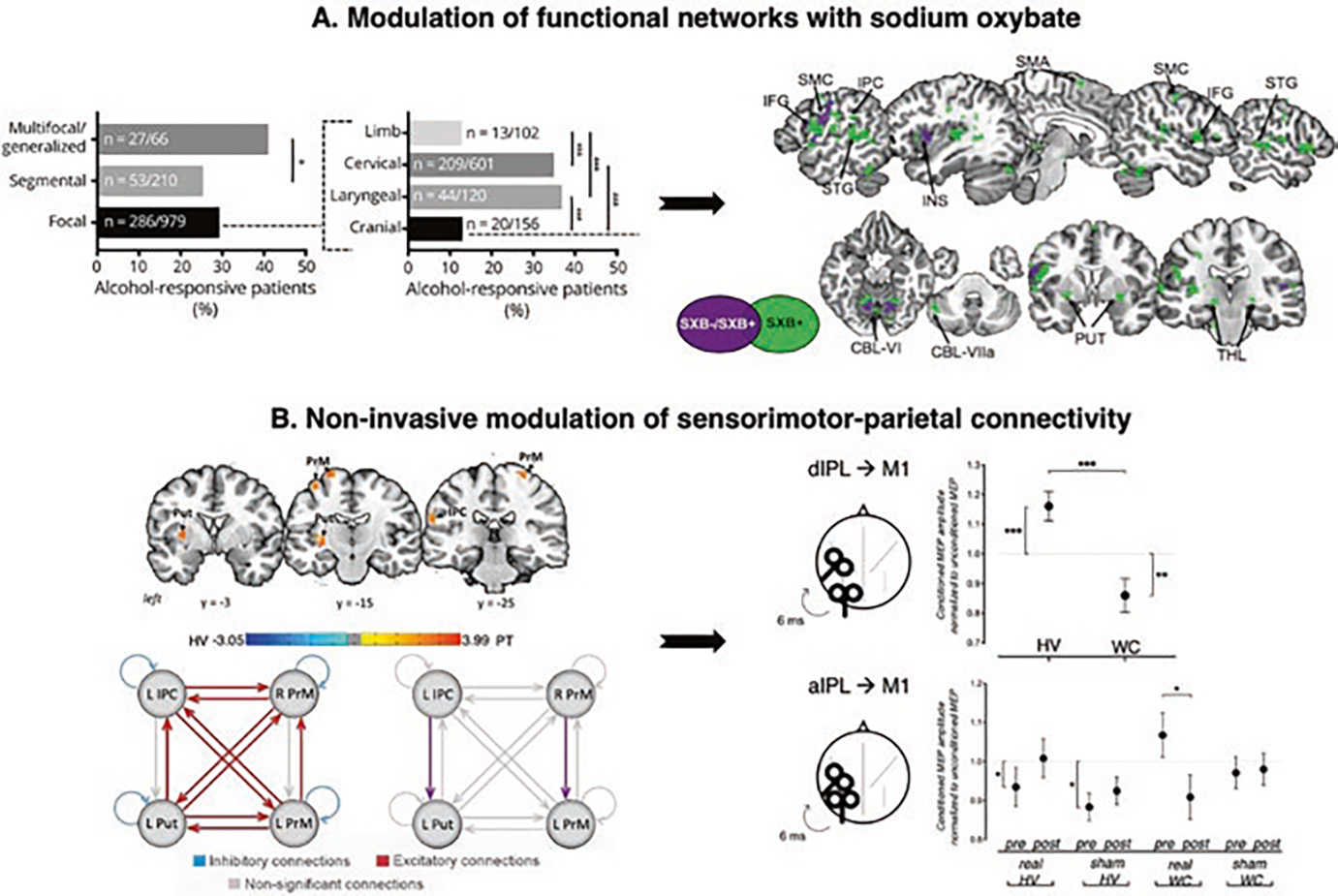
Clinical implications of dystonia as a functional neural network disorder. (a) Alcohol responsiveness in dystonia and the effects of sodium oxybate on brain activity. The left panel shows the alcohol responsiveness across different forms of dystonia (in % of patients in the examined cohort). The black arrow indicates how the understanding of alcohol responsiveness in dystonia influenced the design of the open-label study in laryngeal dystonia using sodium oxybate, a gamma-hydroxybutyric acid that mimics the effects of alcohol. The right panel shows a series of sagittal and axial slices of regions of common (in purple) and distinct (in green) brain activity in drug responders vs. nonresponders during symptomatic speech production. (b) Modulation of sensorimotor-parietal connectivity in focal dystonia. The left panel shows series of coronal brain images with regional alterations in resting-state functional connectivity in patients with laryngeal dystonia compared to healthy subjects. The schematic representation of the results of dynamic causal modeling reveals the direction of abnormal information flow between these altered regions in patients. Excitatory connections (red), inhibitory connections (blue), nonsignificant connections (gray), differences between laryngeal dystonia patients and healthy subjects (purple). The black arrow shows how imaging studies of functional and effective connectivity in dystonia informed the design of noninvasive neuromodulation in these patients. The right panel summarizes the transcranial magnetic stimulation experiment in healthy subjects and patients with writer’s cramp. The panel shows changes in sensorimotor-inferior parietal electrophysiological interaction introduced by real or sham continuous theta-burst stimulation. Abbreviations: M1 motor cortex, dIPL dorsal inferior parietal lobule, aIPL anterior inferior parietal lobule. (Panel (a) adapted from Simonyan et al. [99]. Panel (b) adapted from Battistella G. and K. Simonyan [6] and Merchant et al. [80])
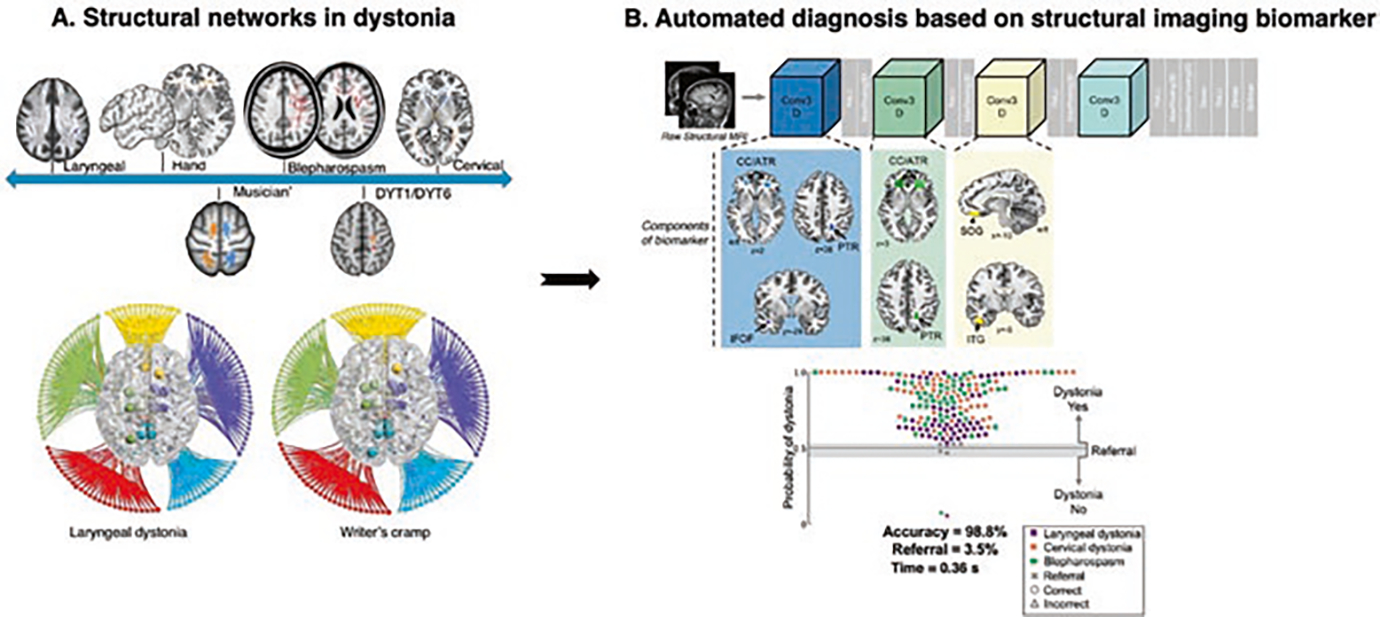
Clinical implications of dystonia as a structural neural network disorder. (a) Structural abnormalities in dystonia: the top panel shows the major microstructural abnormalities across different forms of dystonia. The bottom panel shows the large-scale connectome in focal dystonias. (b) Automated diagnosis of dystonia using DystoniaNet. The automated algorithm identified gray and white matter regions classifying patients with different forms of focal dystonia. The scatterplot shows the accuracy of the algorithm. (Panel (a) adapted from Hanekamp and Simonyan [54]. Panel (b) adapted from Valeriani and Simonyan [109])
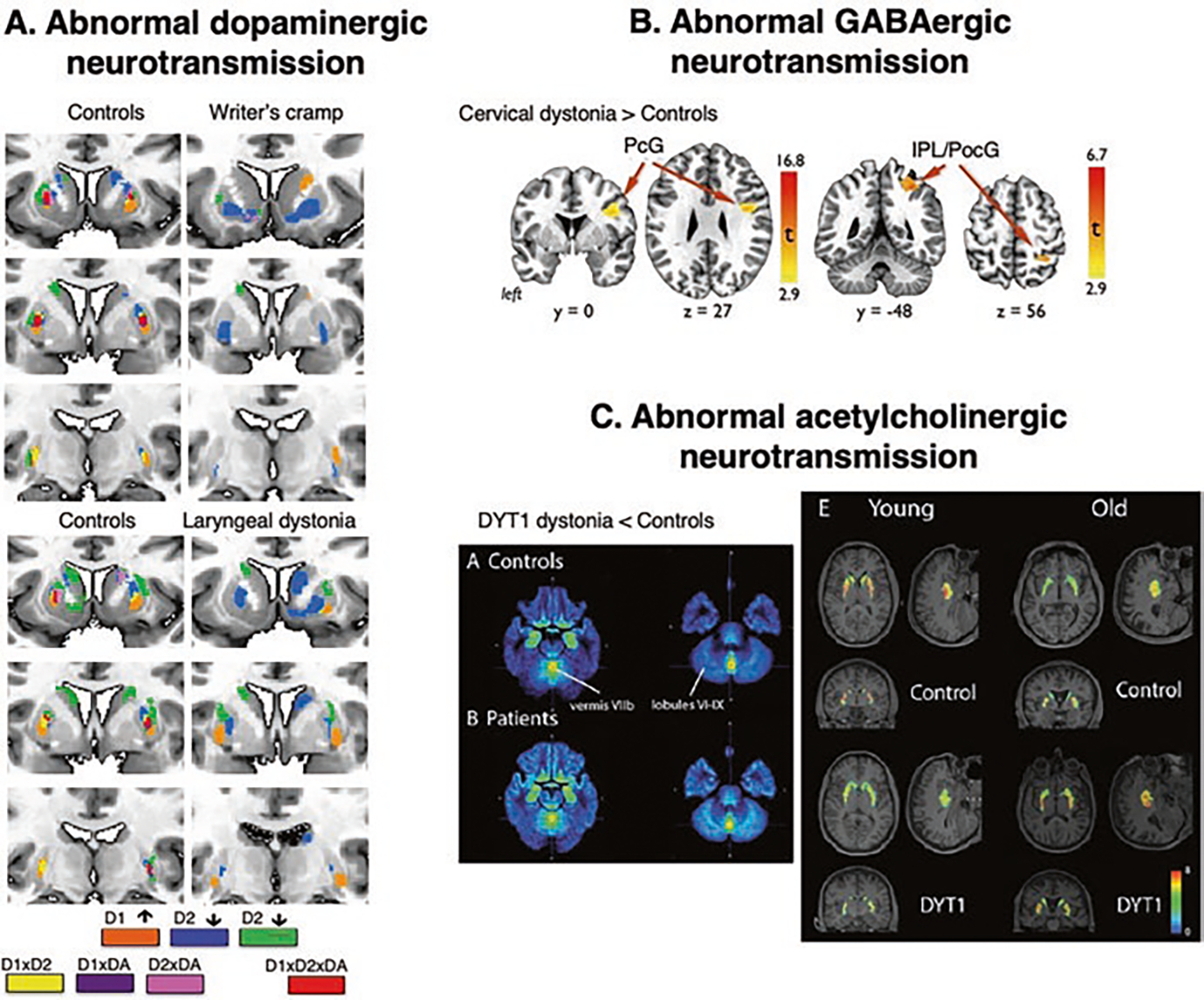
Clinical implications of dystonia as a neurotransmission network disorder. (a) Topological distribution of phasic striatal dopamine in healthy subjects and patients with writer’s cramp and laryngeal dystonia during finger tapping (for hand dystonia) and sentence production (for laryngeal dystonia). Different colors represent receptor-binding regions (D1, D2), dopamine release (DA), and their significant interactions. (b) Distribution of increased GABAA receptor binding in cervical dystonia compared to healthy subjects using [11C] flumazenil radiotracer. (c) Parametric map of decreased vesicular acetylcholine transporter in patients with DYT1 dystonia compared to healthy subjects using 18F-FEOBV-binding ratio and average binding in controls and patients stratified by age. (Panel (a) adapted from Simonyan et al. [98]. Panel (b) adapted from Berman et al. [13]. Panel (c) adapted from Mazere et al. [79])
References
-
- Albanese A, Barnes MP, Bhatia KP, Fernandez-Alvarez E, Filippini G, Gasser T, Krauss JK, Newton A, Rektor I, Savoiardo M, Valls-Solè J. A systematic review on the diagnosis and treatment of primary (idiopathic) dystonia and dystonia plus syndromes: report of an EFNS/MDS-ES Task Force. Eur J Neurol. 2006;13:433–44. - PubMed
-
- Asanuma K, Ma Y, Okulski J, Dhawan V, Chaly T, Carbon M, Bressman SB, Eidelberg D. Decreased striatal D2 receptor binding in non-manifesting carriers of the DYT1 dystonia mutation. Neurology. 2005;64:347–9. - PubMed
-
- Balint B, Mencacci NE, Valente EM, Pisani A, Rothwell J, Jankovic J, Vidailhet M, Bhatia KP. Dystonia. Nat Rev Dis Primers. 2018;4:25. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical