

Do the Revision Rates of Arthroplasty Surgeons Correlate With Postoperative Patient-reported Outcome Measure Scores? A Study From the Australian Orthopaedic Association National Joint Replacement Registry
- PMID: 37339166
- PMCID: PMC10723865
- DOI: 10.1097/CORR.0000000000002737
Do the Revision Rates of Arthroplasty Surgeons Correlate With Postoperative Patient-reported Outcome Measure Scores? A Study From the Australian Orthopaedic Association National Joint Replacement Registry
Abstract
Background: Patient-reported outcome measures (PROMs) are a pragmatic and efficient means to evaluate the functional quality of arthroplasty beyond revision rates, which are used by most joint replacement registries to judge success. The relationship between these two measures of quality-revision rates and PROMs-is unknown, and not every procedure with a poor functional result is revised. It is logical-although still untested-that higher cumulative revision rates correlate inversely with PROMs for individual surgeons; more revisions are associated with lower PROM scores.
Questions/purposes: We used data from a large national joint replacement registry to ask: (1) Does a surgeon's early THA cumulative percent revision (CPR) rate and (2) early TKA CPR rate correlate with the postoperative PROMs of patients undergoing primary THA and TKA, respectively, who have not undergone revision?
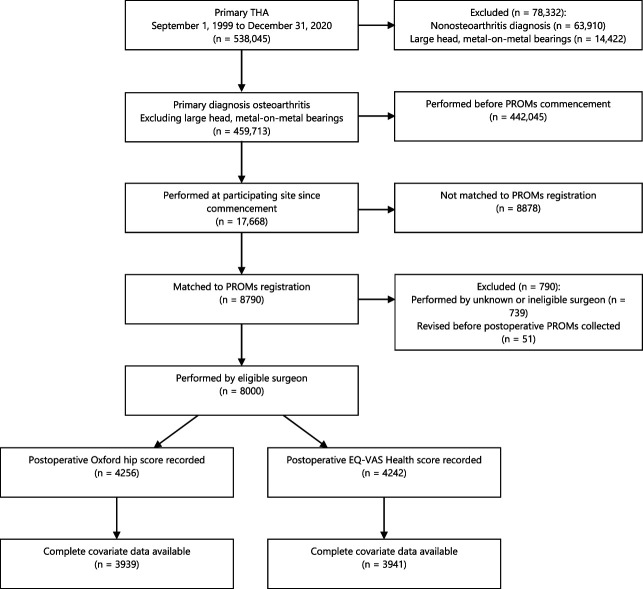
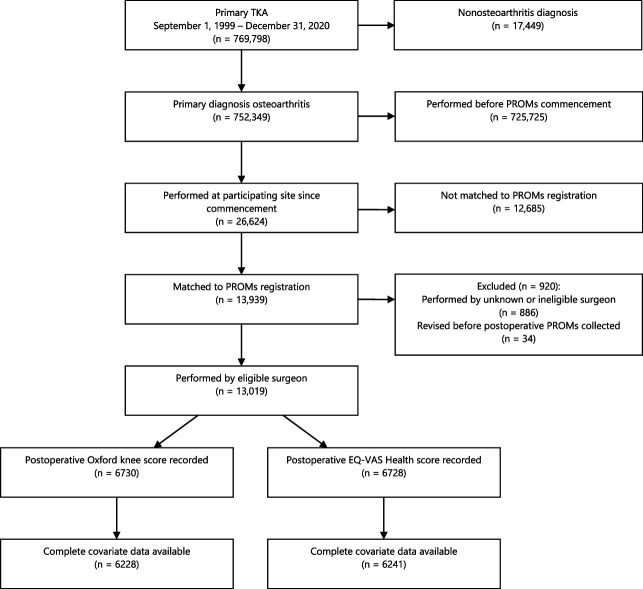
Methods: Elective primary THA and TKA procedures in patients with a primary diagnosis of osteoarthritis that were performed between August 2018 and December 2020 and registered in the Australian Orthopaedic Association National Joint Replacement Registry PROMs program were eligible. THAs and TKAs were eligible for inclusion in the primary analysis if 6-month postoperative PROMs were available, the operating surgeon was clearly identified, and the surgeon had performed at least 50 primary THAs or TKAs. Based on the inclusion criteria, 17,668 THAs were performed at eligible sites. We excluded 8878 procedures that were not matched to the PROMs program, leaving 8790 procedures. A further 790 were excluded because they were performed by unknown or ineligible surgeons or were revised, leaving 8000 procedures performed by 235 eligible surgeons, including 4256 (53%; 3744 cases of missing data) patients who had postoperative Oxford Hip Scores and 4242 (53%; 3758 cases of missing data) patients who had a postoperative EQ-VAS score recorded. Complete covariate data were available for 3939 procedures for the Oxford Hip Score and for 3941 procedures for the EQ-VAS. A total of 26,624 TKAs were performed at eligible sites. We excluded 12,685 procedures that were not matched to the PROMs program, leaving 13,939 procedures. A further 920 were excluded because they were performed by unknown or ineligible surgeons, or because they were revisions, leaving 13,019 procedures performed by 276 eligible surgeons, including 6730 (52%; 6289 cases of missing data) patients who had had postoperative Oxford Knee Scores and 6728 (52%; 6291 cases of missing data) patients who had a postoperative EQ-VAS score recorded. Complete covariate data were available for 6228 procedures for the Oxford Knee Score and for 6241 procedures for the EQ-VAS. The Spearman correlation between the operating surgeon's 2-year CPR and 6-month postoperative EQ-VAS Health and Oxford Hip or Oxford Knee Score was evaluated for THA and TKA procedures where a revision had not been performed. Associations between postoperative Oxford and EQ-VAS scores and a surgeon's 2-year CPR were estimated based on multivariate Tobit regressions and a cumulative link model with a probit link, adjusting for patient age, gender, ASA score, BMI category, preoperative PROMs, as well as surgical approach for THA. Missing data were accounted for using multiple imputation, with models assuming they were missing at random and a worst-case scenario.
Results: Of the eligible THA procedures, postoperative Oxford Hip Score and surgeon 2-year CPR were correlated so weakly as to be clinically irrelevant (Spearman correlation ρ = -0.09; p < 0.001), and the correlation with postoperative EQ-VAS was close to zero (ρ = -0.02; p = 0.25). Of the eligible TKA procedures, postoperative Oxford Knee Score and EQ-VAS and surgeon 2-year CPR were correlated so weakly as to be clinically irrelevant (ρ = -0.04; p = 0.004 and ρ = 0.03; p = 0.006, respectively). All models accounting for missing data found the same result.
Conclusion: A surgeon's 2-year CPR did not exhibit a clinically relevant correlation with PROMs after THA or TKA, and all surgeons had similar postoperative Oxford scores. PROMs, revision rates, or both may be inaccurate or imperfect indicators of successful arthroplasty. Missing data may limit the findings of this study, although the results were consistent under a variety of different missing data scenarios. Innumerable factors contribute to arthroplasty results, including patient-related variables, differences in implant design, and the technical quality of the procedure. PROMs and revision rates may be analyzing two different facets of function after arthroplasty. Although surgeon variables are associated with revision rates, patient factors may exert a stronger influence on functional outcomes. Future research should identify variables that correlate with functional outcome. Additionally, given the gross level of function that Oxford scores record, outcome measures that can identify clinically meaningful functional differences are required. The use of Oxford scores in national arthroplasty registries may rightfully be questioned.
Level of evidence: Level III, therapeutic study.
Copyright © 2023 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Figures
Comment in
-
CORR Insights®: Do the Revision Rates of Arthroplasty Surgeons Correlate With Postoperative Patient-reported Outcome Measure Scores? A Study From the Australian Orthopaedic Association National Joint Replacement Registry.Clin Orthop Relat Res. 2024 Jan 1;482(1):113-114. doi: 10.1097/CORR.0000000000002796. Epub 2023 Jul 28. Clin Orthop Relat Res. 2024. PMID: 37506050 Free PMC article. No abstract available.
References
-
- AOANJRR. Hip, knee & shoulder arthroplasty: annual report 2019 . Available at https://aoanjrr.sahmri.com/annual-reports-2019. Accessed November 14, 2020.
-
- Austin PC, Escobar M, Kopec JA. The use of the Tobit model for analyzing measures of health status. Qual Life Res. 2000;9:901-910. - PubMed
-
- Bowling A. What things are important in people's lives? A survey of the public's judgements to inform scales of health related quality of life. Soc Sci Med. 1995;41:1447-1462. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
