

Subclinical atherosclerosis and accelerated epigenetic age mediated by inflammation: a multi-omics study
- PMID: 37339167
- PMCID: PMC10393076
- DOI: 10.1093/eurheartj/ehad361
Subclinical atherosclerosis and accelerated epigenetic age mediated by inflammation: a multi-omics study
Abstract
Aims: Epigenetic age is emerging as a personalized and accurate predictor of biological age. The aim of this article is to assess the association of subclinical atherosclerosis with accelerated epigenetic age and to investigate the underlying mechanisms mediating this association.
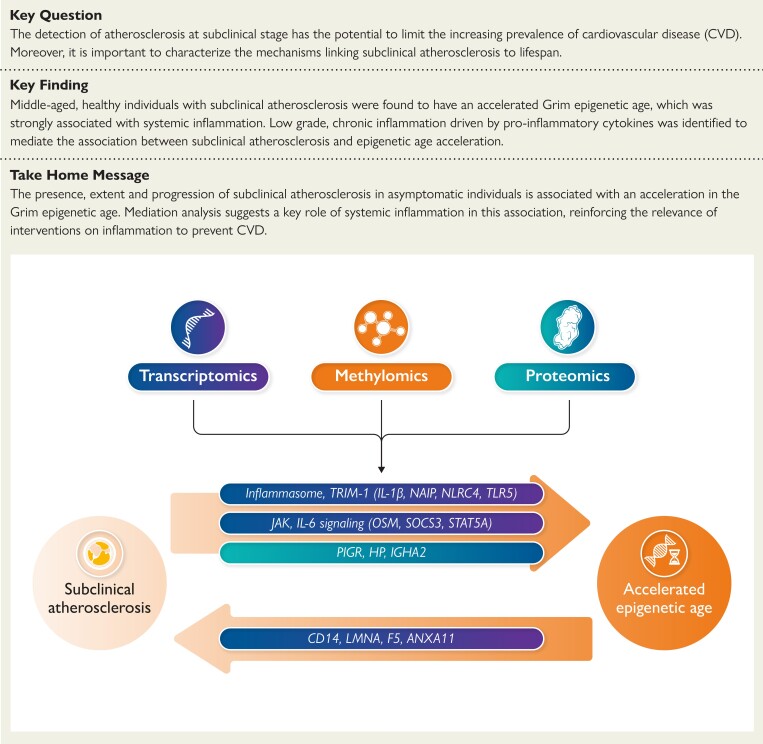
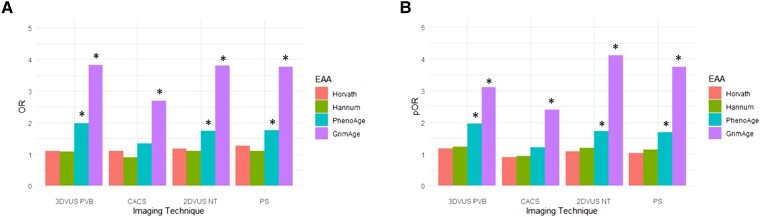
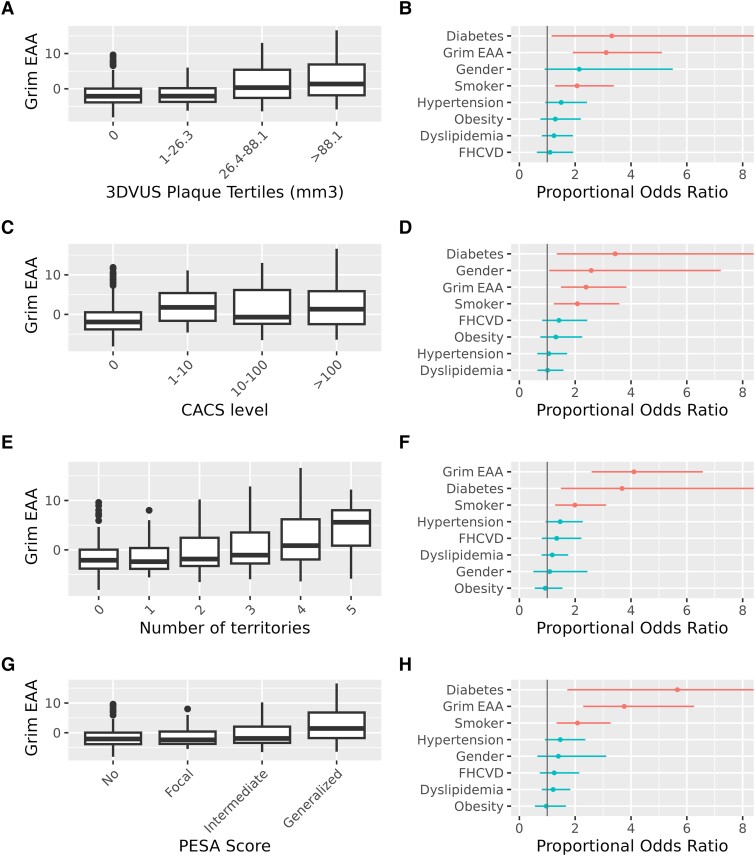
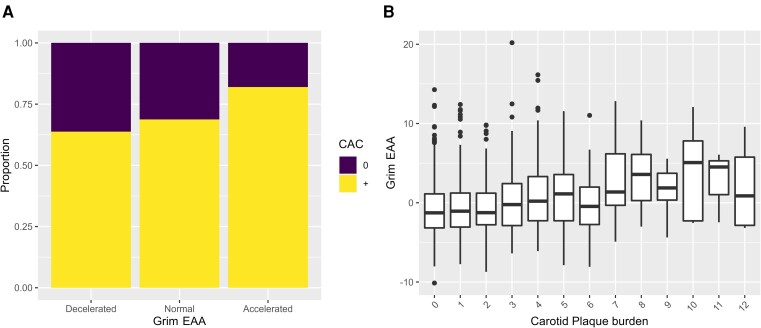
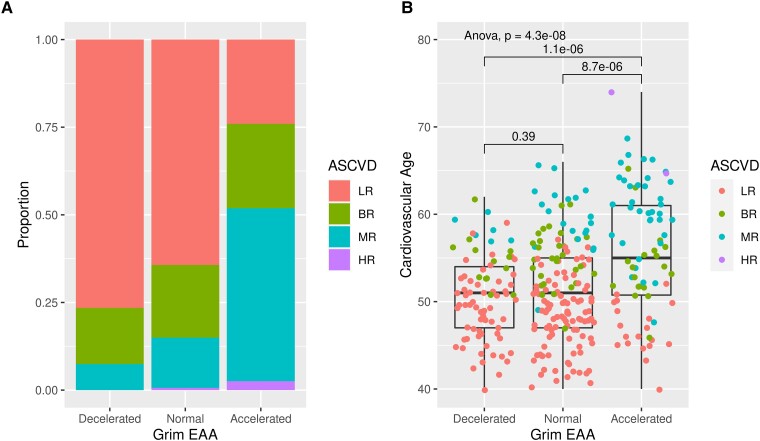
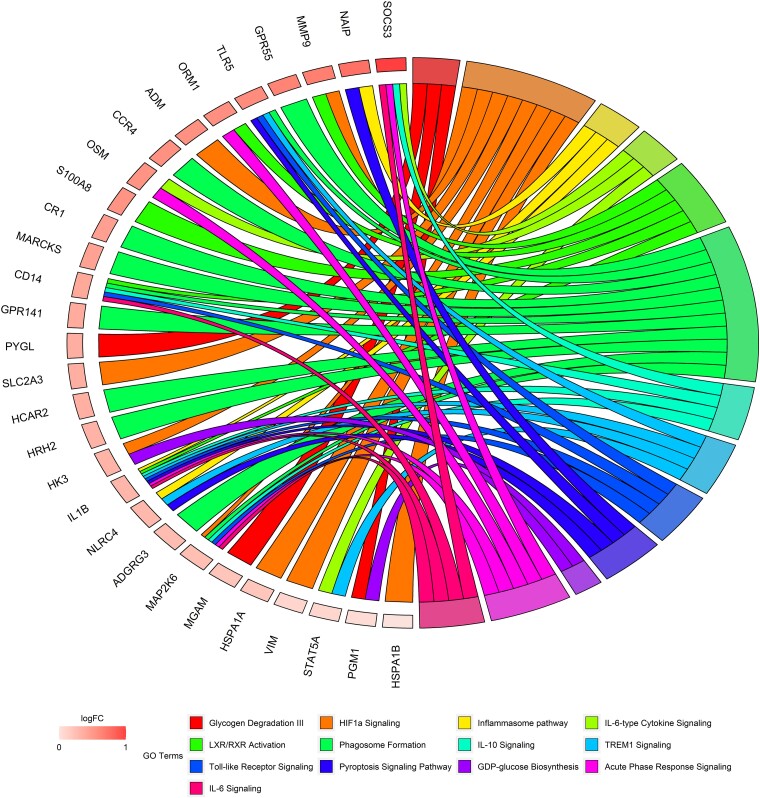
Methods and results: Whole blood methylomics, transcriptomics, and plasma proteomics were obtained for 391 participants of the Progression of Early Subclinical Atherosclerosis study. Epigenetic age was calculated from methylomics data for each participant. Its divergence from chronological age is termed epigenetic age acceleration. Subclinical atherosclerosis burden was estimated by multi-territory 2D/3D vascular ultrasound and by coronary artery calcification. In healthy individuals, the presence, extension, and progression of subclinical atherosclerosis were associated with a significant acceleration of the Grim epigenetic age, a predictor of health and lifespan, regardless of traditional cardiovascular risk factors. Individuals with an accelerated Grim epigenetic age were characterized by an increased systemic inflammation and associated with a score of low-grade, chronic inflammation. Mediation analysis using transcriptomics and proteomics data revealed key pro-inflammatory pathways (IL6, Inflammasome, and IL10) and genes (IL1B, OSM, TLR5, and CD14) mediating the association between subclinical atherosclerosis and epigenetic age acceleration.
Conclusion: The presence, extension, and progression of subclinical atherosclerosis in middle-aged asymptomatic individuals are associated with an acceleration in the Grim epigenetic age. Mediation analysis using transcriptomics and proteomics data suggests a key role of systemic inflammation in this association, reinforcing the relevance of interventions on inflammation to prevent cardiovascular disease.
Trial registration: ClinicalTrials.gov NCT01410318.
Keywords: Epigenetic age acceleration; Methylomics; Proteomics; Subclinical atherosclerosis; Systemic inflammation; Transcriptomics.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest None declared.
Figures
Comment in
-
A Grim link: the association between subclinical atherosclerosis and epigenetic age.Eur Heart J. 2023 Aug 1;44(29):2710-2712. doi: 10.1093/eurheartj/ehad326. Eur Heart J. 2023. PMID: 37309608 Free PMC article.
References
-
- Fernández-Friera L, Peñalvo JL, Fernández-Ortiz A, Ibañez B, López-Melgar B, Laclaustra M, et al. . Prevalence, vascular distribution, and multiterritorial extent of subclinical atherosclerosis in a middle-aged cohort: the PESA (Progression of Early Subclinical Atherosclerosis) study. Circulation 2015;131:2104–2113. 10.1161/CIRCULATIONAHA.114.014310 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
