

Indications, Resource Allocation, and Outcomes Associated with Ex-Utero Intrapartum Treatment Procedures: A North American Fetal Therapy Network Survey
- PMID: 37339615
- PMCID: PMC10614236
- DOI: 10.1159/000531615
Indications, Resource Allocation, and Outcomes Associated with Ex-Utero Intrapartum Treatment Procedures: A North American Fetal Therapy Network Survey
Abstract
Introduction: Neonates with cardiorespiratory compromise at delivery are at substantial risk of hypoxic neurologic injury and death. Though mitigation strategies such as ex-utero intrapartum treatment (EXIT) exist, the competing interests of neonatal beneficence, maternal non-maleficence, and just distribution of resources require consideration. Due to the rarity of these entities, there are few systematic data to guide evidence-based standards. This multi-institutional, interdisciplinary approach aims to elucidate the current scope of diagnoses that might be considered for such treatments and examine if treatment allocation and/or outcomes could be improved.
Methods: After IRB approval, a survey investigating diagnoses appropriate for EXIT consultation and procedure, variables within each diagnosis, occurrence of maternal and neonatal adverse outcomes, and instances of suboptimal resource allocation in the last decade was sent to all North American Fetal Treatment Network center representatives. One response was recorded per center.
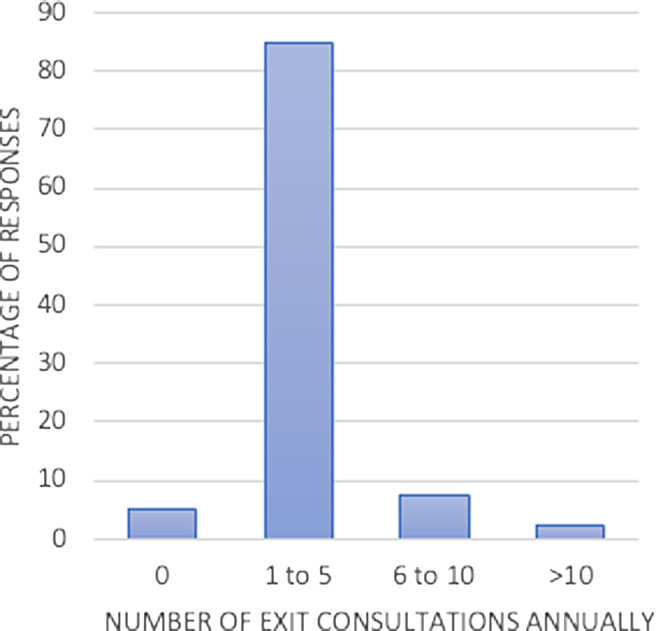
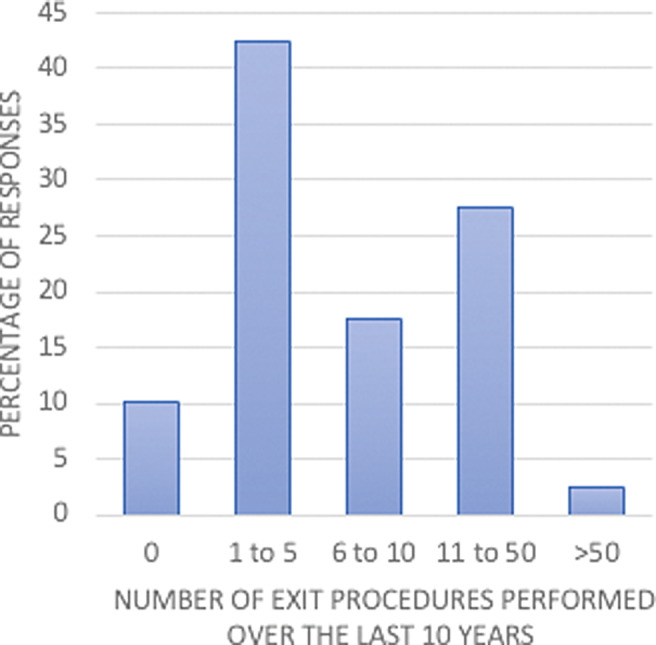
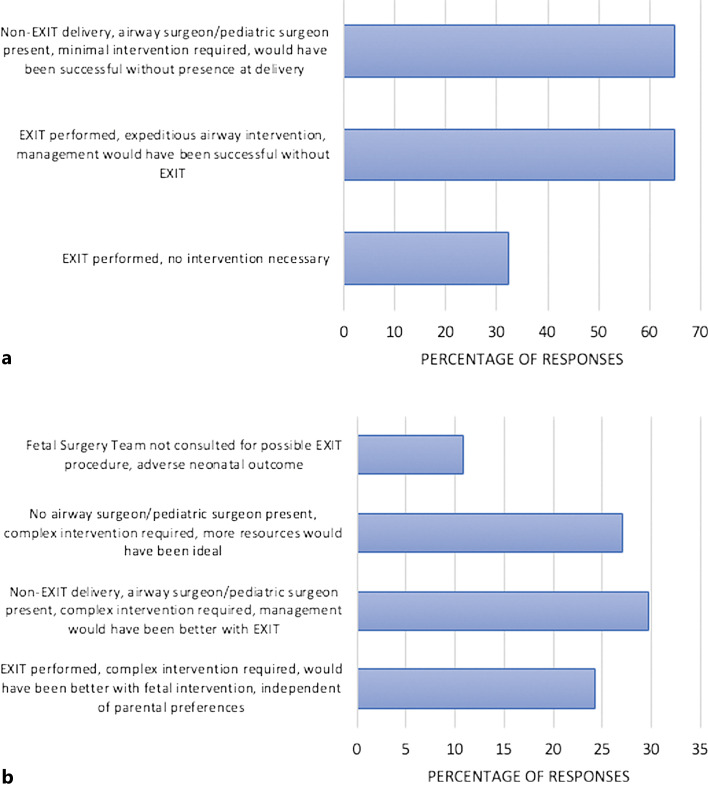
Results: We received a 91% response rate and all but one center offer EXIT. Most centers (34/40, 85%) performed 1-5 EXIT consultations per year and 17/40 (42.5%) centers performed 1-5 EXIT procedures in the last 10 years. The diagnoses with the highest degree of agreement between centers surveyed to justify consultation for EXIT are head and neck mass (100%), congenital high airway obstruction (90%), and craniofacial skeletal conditions (82.5%). Maternal adverse outcomes were noted in 7.5% of centers while neonatal adverse outcomes in 27.5%. A large percentage of centers report cases of suboptimal selection for risk mitigation procedures and several centers experienced adverse neonatal and maternal outcomes.
Conclusion: This study captures the scope of EXIT indications and is the first to demonstrate the mismatch in resource allocation for this population. Further, it reports on attributable adverse outcomes. Given suboptimal allocation and adverse outcomes, further examination of indications, outcomes, and resource use is justified to drive evidence-based protocols.
Keywords: Ex utero intrapartum treatment; Fetal surgery; Resource allocation.
© 2023 S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Maternal and obstetric outcomes after Ex-Utero Intrapartum Treatment (EXIT): a single center experience.BMC Pregnancy Childbirth. 2023 Dec 2;23(1):831. doi: 10.1186/s12884-023-06129-9. BMC Pregnancy Childbirth. 2023. PMID: 38042795 Free PMC article.
-
A review of the EXIT (Ex utero Intrapartum Treatment) procedure.J Obstet Gynaecol. 2010 Jan;30(1):1-5. doi: 10.3109/01443610903281656. J Obstet Gynaecol. 2010. PMID: 20121493 Review.
-
Prenatal Imaging Findings Predict Obstructive Fetal Airways Requiring EXIT.Laryngoscope. 2021 Apr;131(4):E1357-E1362. doi: 10.1002/lary.28959. Epub 2020 Aug 8. Laryngoscope. 2021. PMID: 32770766
-
Fetal Laryngoscopy and Endoscopic Tracheal Intubation to Avoid ex utero Intrapartum Treatment in the Management of Fetuses with Suspected Airway Obstruction.Fetal Diagn Ther. 2023;50(6):472-479. doi: 10.1159/000533348. Epub 2023 Aug 4. Fetal Diagn Ther. 2023. PMID: 37544292
-
Ex utero intrapartum treatment (EXIT) for fetal neck masses: A tertiary center experience and literature review.Int J Pediatr Otorhinolaryngol. 2019 Dec;127:109642. doi: 10.1016/j.ijporl.2019.109642. Epub 2019 Aug 13. Int J Pediatr Otorhinolaryngol. 2019. PMID: 31479918
Cited by
-
Perinatal Airway Management Mandibular Anomalies: A National Inpatient Cohort Analysis.Laryngoscope. 2025 May;135 Suppl 3(Suppl 3):S1-S12. doi: 10.1002/lary.31699. Epub 2024 Aug 14. Laryngoscope. 2025. PMID: 39140255 Free PMC article.
-
Neonatal Tracheal Intubation in the NICU: A Literature Review.Healthcare (Basel). 2025 May 24;13(11):1242. doi: 10.3390/healthcare13111242. Healthcare (Basel). 2025. PMID: 40508856 Free PMC article. Review.
-
The Ex-utero intrapartum treatment procedure: a narrative review.Front Pediatr. 2025 Jul 17;13:1601963. doi: 10.3389/fped.2025.1601963. eCollection 2025. Front Pediatr. 2025. PMID: 40746351 Free PMC article. Review.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
