

Distal Versus Total D2-Gastrectomy for Gastric Cancer: a Secondary Analysis of Surgical and Oncological Outcomes Including Quality of Life in the Multicenter Randomized LOGICA-Trial
- PMID: 37340107
- PMCID: PMC10511620
- DOI: 10.1007/s11605-023-05683-z
Distal Versus Total D2-Gastrectomy for Gastric Cancer: a Secondary Analysis of Surgical and Oncological Outcomes Including Quality of Life in the Multicenter Randomized LOGICA-Trial
Abstract
Background: Distal gastrectomy (DG) for gastric cancer can cause less morbidity than total gastrectomy (TG), but may compromise radicality. No prospective studies administered neoadjuvant chemotherapy, and few assessed quality of life (QoL).
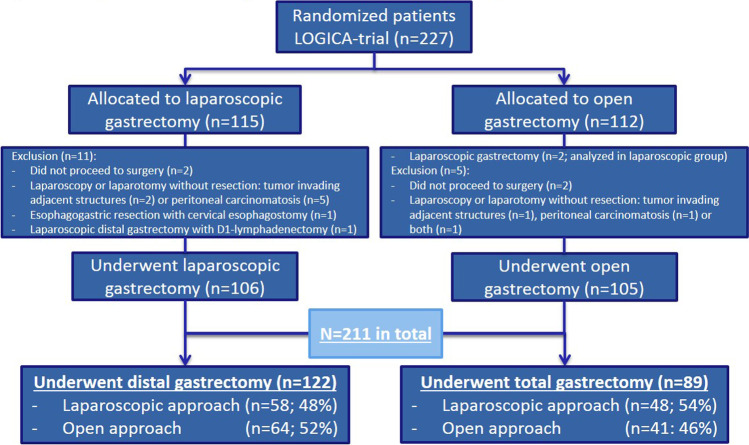
Methods: The multicenter LOGICA-trial randomized laparoscopic versus open D2-gastrectomy for resectable gastric adenocarcinoma (cT1-4aN0-3bM0) in 10 Dutch hospitals. This secondary LOGICA-analysis compared surgical and oncological outcomes after DG versus TG. DG was performed for non-proximal tumors if R0-resection was deemed achievable, TG for other tumors. Postoperative complications, mortality, hospitalization, radicality, nodal yield, 1-year survival, and EORTC-QoL-questionnaires were analyzed using Χ2-/Fisher's exact tests and regression analyses.
Results: Between 2015 and 2018, 211 patients underwent DG (n = 122) or TG (n = 89), and 75% of patients underwent neoadjuvant chemotherapy. DG-patients were older, had more comorbidities, less diffuse type tumors, and lower cT-stage than TG-patients (p < 0.05). DG-patients experienced fewer overall complications (34% versus 57%; p < 0.001), also after correcting for baseline differences, lower anastomotic leakage (3% versus 19%), pneumonia (4% versus 22%), atrial fibrillation (3% versus 14%), and Clavien-Dindo grading compared to TG-patients (p < 0.05), and demonstrated shorter median hospital stay (6 versus 8 days; p < 0.001). QoL was better after DG (statistically significant and clinically relevant) in most 1-year postoperative time points. DG-patients showed 98% R0-resections, and similar 30-/90-day mortality, nodal yield (28 versus 30 nodes; p = 0.490), and 1-year survival after correcting for baseline differences (p = 0.084) compared to TG-patients.
Conclusions: If oncologically feasible, DG should be preferred over TG due to less complications, faster postoperative recovery, and better QoL while achieving equivalent oncological effectiveness. Distal D2-gastrectomy for gastric cancer resulted in less complications, shorter hospitalization, quicker recovery and better quality of life compared to total D2-gastrectomy, whereas radicality, nodal yield and survival were similar.
Trial registration: ClinicalTrials.gov NCT02248519.
Keywords: Gastrectomy; Gastric cancer; Patient selection; Postoperative complications; Quality of life.
© 2023. The Author(s).
Conflict of interest statement
Richard van Hillegersberg: consulting or advisory role: intuitive surgical, Medtronic. Jelle Ruurda: consulting or advisory role: intuitive surgical. Lodewijk Brosens: advisory role: Bristol Myers Squibb. Grard Nieuwenhuijzen: consulting or advisory role: Medtronic. The other authors have no disclosures. All authors declared no conflicts of interest.
Figures
References
-
- Al-Batran SE, Homann N, Pauligk C, Goetze TO, Meiler J, Kasper S, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a ra. Lancet. 2019;393:1948–1957. doi: 10.1016/S0140-6736(18)32557-1. - DOI - PubMed
-
- Cunningham D, Allum WH, Stenning SP, Thompson JN, Van de Velde CJ, Nicolson M, Scarffe JH, Lofts FJ, Falk SJ, Iveson TJ, Smith DB, Langley RE, Verma M, Weeden S, Chua YJMTP. Perioperative Chemotherapy versus Surgery Alone for Resectable Gastroesophageal Cancer. N Engl J Med. 2006;355:11–20. doi: 10.1056/NEJMoa055531. - DOI - PubMed
-
- Vereniging van Integrale Kankercentra. Dutch national guidelines. Diagnostics, treatment and follow-up of gastric cancer. Version 2.2. last updated: 2017–03–01. 2017:1-162.
-
- Gertsen EC, Brenkman HJF, Haverkamp L, Read M, Ruurda JP, van Hillegersberg R. Worldwide Practice in Gastric Cancer Surgery: A 6-Year Update. Dig Surg 2021:1–9. 10.1159/000515768. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
