

Bacterial shedding and serologic responses following an outbreak of Salmonella Typhi in an endemic cohort
- PMID: 37340341
- PMCID: PMC10280929
- DOI: 10.1186/s12879-023-08385-8
Bacterial shedding and serologic responses following an outbreak of Salmonella Typhi in an endemic cohort
Abstract
Background: Salmonella enterica serovar Typhi (Salmonella Typhi) is the cause of typhoid fever. Salmonella Typhi may be transmitted through shedding in the stool, which can continue after recovery from acute illness. Shedding is detected by culturing stool, which is challenging to co-ordinate at scale. We hypothesised that sero-surveillance would direct us to those shedding Salmonella Typhi in stool following a typhoid outbreak.
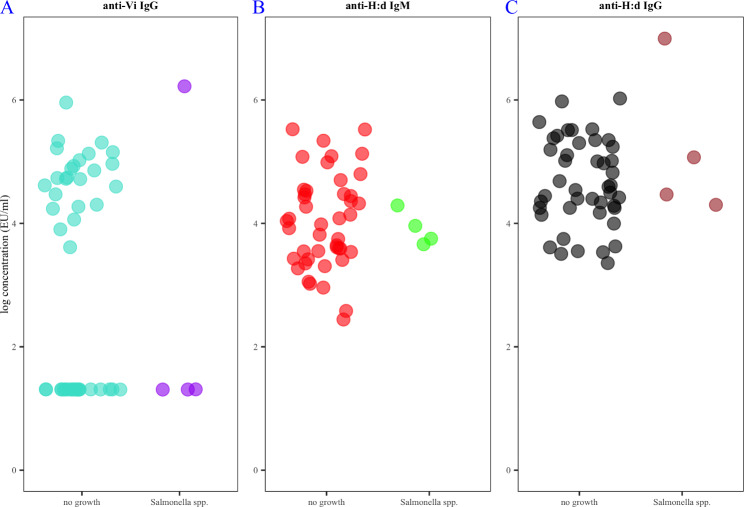
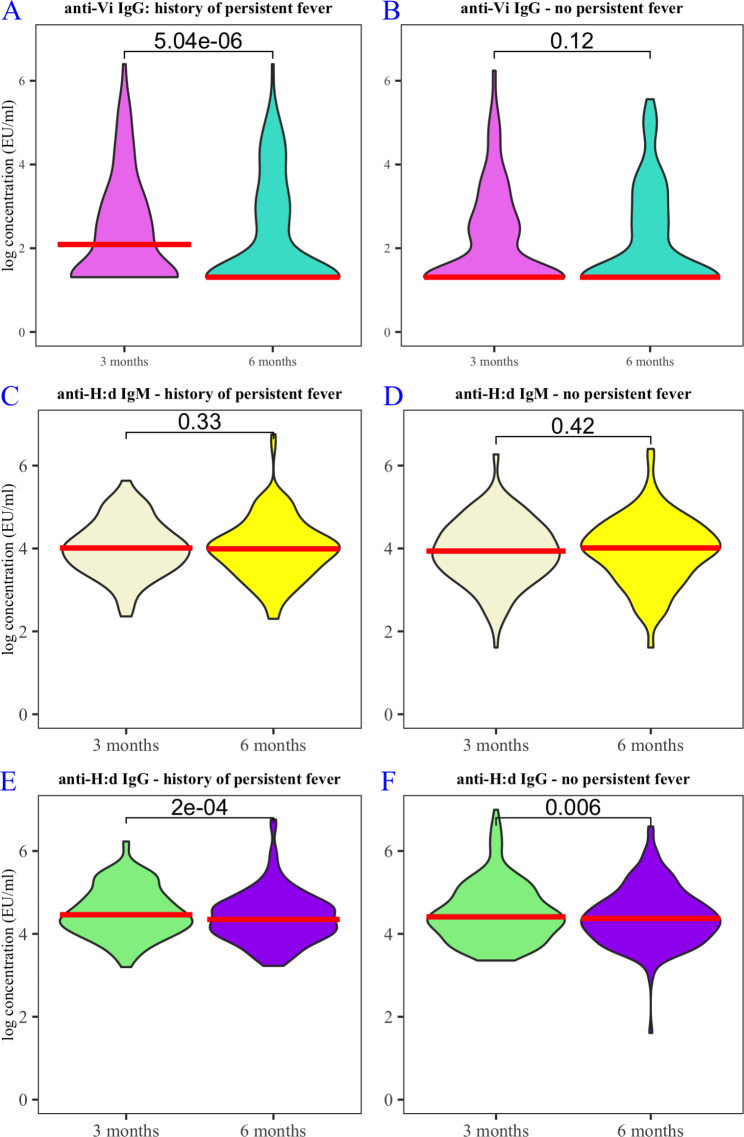
Methods: In 2016 a typhoid outbreak affected one in four residents of a Nursing School in Malosa, Malawi. The Department of Health asked for assistance to identify nursing students that might spread the outbreak to other health facilities. We measured IgG antibody titres against Vi capsular polysaccharide (anti-Vi IgG) and IgM / IgG antibodies against H:d flagellin (anti-H:d) three and six months after the outbreak. We selected participants in the highest and lowest deciles for anti-Vi IgG titre (measured at visit one) and obtained stool for Salmonella culture and PCR. All participants reported whether they had experienced fever persisting for three days or more during the outbreak (in keeping with the WHO definitions of 'suspected typhoid'). We tested for salmonellae in the Nursing School environment.
Results: We obtained 320 paired serum samples from 407 residents. We cultured stool from 25 residents with high anti-Vi IgG titres and 24 residents with low titres. We did not recover Salmonella Typhi from stool; four stool samples yielded non-typhoidal salmonellae; one sample produced a positive PCR amplification for a Salmonella Typhi target. Median anti-Vi and anti-H:d IgG titres fell among participants who reported persistent fever. There was a smaller fall in anti-H:d IgG titres among participants who did not report persistent fever. Non-typhoidal salmonellae were identified in water sampled at source and from a kitchen tap.
Conclusion: High titres of anti-Vi IgG did not identify culture-confirmed shedding of Salmonella Typhi. There was a clear serologic signal of recent typhoid exposure in the cohort, represented by waning IgG antibody titres over time. The presence of non-typhoidal salmonellae in drinking water indicates sub-optimal sanitation. Developing methods to detect and treat shedding remains an important priority to complement typhoid conjugate vaccination in efforts to achieve typhoid elimination.
Keywords: Outbreak; Salmonella Typhi; Sero-surveillance; Shedding; Typhoid.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Specific and cross-reactive immune response to oral Salmonella Typhi Ty21a and parenteral Vi capsular polysaccharide typhoid vaccines administered concomitantly.Vaccine. 2015 Jan 9;33(3):451-8. doi: 10.1016/j.vaccine.2014.11.030. Epub 2014 Nov 26. Vaccine. 2015. PMID: 25433216
-
The Impact of Vaccination and Prior Exposure on Stool Shedding of Salmonella Typhi and Salmonella Paratyphi in 6 Controlled Human Infection Studies.Clin Infect Dis. 2019 Apr 8;68(8):1265-1273. doi: 10.1093/cid/ciy670. Clin Infect Dis. 2019. PMID: 30252031 Free PMC article.
-
Evaluation of TUBEX-TF and OnSite Typhoid IgG/IgM Combo rapid tests to detect Salmonella enterica serovar Typhi infection during a typhoid outbreak in Harare, Zimbabwe.BMC Res Notes. 2015 Feb 24;8:50. doi: 10.1186/s13104-015-1015-1. BMC Res Notes. 2015. PMID: 25890321 Free PMC article.
-
Significance of Vi Negative Isolates of Salmonella Enterica Serovar Typhi.Adv Exp Med Biol. 2018;1052:9-18. doi: 10.1007/978-981-10-7572-8_2. Adv Exp Med Biol. 2018. PMID: 29785477 Review.
-
Salmonella enterica serovar Typhi and gallbladder cancer: a case-control study and meta-analysis.Cancer Med. 2016 Nov;5(11):3310-3235. doi: 10.1002/cam4.915. Epub 2016 Oct 11. Cancer Med. 2016. PMID: 27726295 Free PMC article. Review.
Cited by
-
Typhoid Fever and Non-typhoidal Salmonella Outbreaks: A Portrait of Regional Socioeconomic Inequalities in Brazil.Curr Microbiol. 2024 Jan 9;81(2):57. doi: 10.1007/s00284-023-03559-8. Curr Microbiol. 2024. PMID: 38196058
References
-
- Hendriksen RS, Leekitcharoenphon P, Lukjancenko O, Lukwesa-Musyani C, Tambatamba B, Mwaba J, et al. Genomic signature of multidrug-resistant Salmonella enterica serovar Typhi isolates related to a massive outbreak in Zambia between 2010 and 2012. J Clin Microbiol. 2015;53(1):262–72. doi: 10.1128/JCM.02026-14. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
