

Needlescopic sutureless repair of congenital inguinal hernia: A randomized controlled study
- PMID: 37341905
- PMCID: PMC10710381
- DOI: 10.1007/s13304-023-01566-9
Needlescopic sutureless repair of congenital inguinal hernia: A randomized controlled study
Abstract
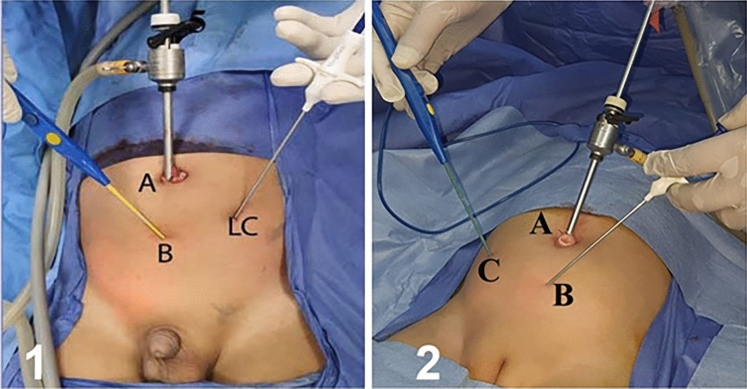
Congenital inguinal hernia [CIH] can be treated laparoscopically using various methods documented in the literature. Many authors have recommended dividing the sac and stitching peritoneal defects. Other studies claimed that peritoneal disconnection alone is sufficient. In this study, the feasibility, operative time, recurrence rate, and other postoperative complications of needlescopic disconnection of the CIH sac with or without peritoneal defect suturing were compared. A prospective controlled randomized trial was conducted between January 2020 and December 2022. Two hundred and thirty patients who met the study requirements were included. Patients were assigned at random to either Group A or Group B. A group of 116 patients (Group A) had needlescopic separation of the neck of the sac and peritoneal defect closure. The remaining 114 patients (Group B) underwent needlescopic separation without peritoneal defect closure (Sutureless group). A total of 260 hernial defects in 230 patients were repaired using needlescopic disconnection with or without suturing of the defect. There were 89 females (38.7%) and 141 males (61.3%), with a mean age of 5.14 ± 2.79 years. In Group A, the mean operation time was 27.98 ± 2.89 for a unilateral hernia and 37.29 ± 4.68 for a bilateral one, whereas, in Group B, the mean operation time was 20.37 ± 2.37 and 23.38 ± 2.22 for a unilateral and bilateral hernia, respectively. In terms of the operating time, whether unilateral or bilateral, there was a significant difference between the groups. There was no significant difference between groups A and B in the mean Internal Ring Diameter [IRD], which was 1.21 ± 0.18 cm in group A and 1.19 ± 0.11 cm in group B. Throughout the follow-up period, there was no postoperative hydrocele formation, recurrence, iatrogenic ascending of the testes, or testicular atrophy. All patients had nearly invisible scars with no keloid development at 3 months follow-up. Needlescopically separating the hernia sac without stitching the peritoneal defect is feasible, safe, and less invasive. It provides outstanding cosmetic results with a short operative time and no recurrence.
Keywords: Diathermy probe; Epidural needle; Infant and children; Mediflex; Needlescopic; Separation.
© 2023. The Author(s).
Conflict of interest statement
All the authors; Prof. Rafik Shalaby, Dr. Mohamed Abdelmaboud, Prof. Mohammad Daboos, Dr. Yousef Mohamed, Prof. Ahmed Abdelghafar Helal, Prof. Ibrahim Gamman) have no conflicts of interest or financial ties to disclose.
Figures



References
-
- Coran AG, Caldamone A, Adzick NS, Krummel TM, Laberge JM, Shamberger R. Pediatric surgery e-book. Elsevier Health Sciences. 2012;76:985–1002.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
