

Characterization of cerebrospinal fluid (CSF) microbiota at the time of initial surgical intervention for children with hydrocephalus
- PMID: 37342995
- PMCID: PMC10284395
- DOI: 10.1371/journal.pone.0280682
Characterization of cerebrospinal fluid (CSF) microbiota at the time of initial surgical intervention for children with hydrocephalus
Abstract
Objective: To characterize the microbiota of the cerebrospinal fluid (CSF) from children with hydrocephalus at the time of initial surgical intervention.
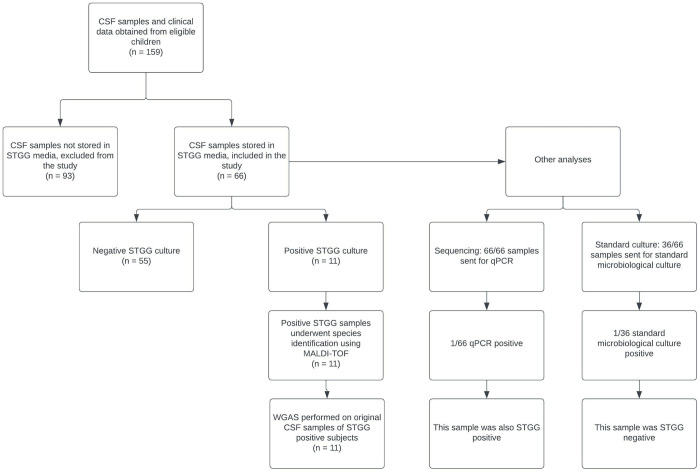
Study design: CSF was obtained at initial surgical intervention. One aliquot was stored in skim milk-tryptone-glucose-glycerol (STGG) medium and the second was unprocessed; both were then stored at -70°C. Bacterial growth for CSF samples stored in STGG were subsequently characterized using aerobic and anaerobic culture on blood agar and MALDI-TOF sequencing. All unprocessed CSF samples underwent 16S quantitative polymerase chain reaction (qPCR) sequencing, and a subset underwent standard clinical microbiological culture. CSF with culture growth (either after storage in STGG or standard clinical) were further analyzed using whole-genome amplification sequencing (WGAS).
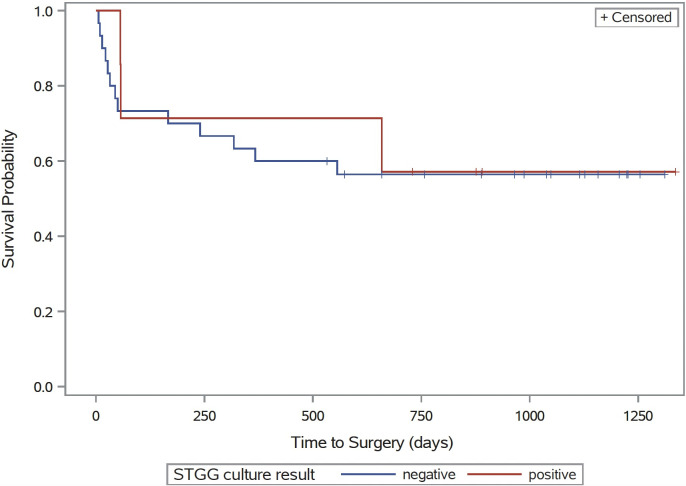
Results: 11/66 (17%) samples stored in STGG and 1/36 (3%) that underwent standard clinical microbiological culture demonstrated bacterial growth. Of the organisms present, 8 were common skin flora and 4 were potential pathogens; only 1 was also qPCR positive. WGAS findings and STGG culture findings were concordant for only 1 sample, identifying Staphylococcus epidermidis. No significant difference in time to second surgical intervention was observed between the STGG culture-positive and negative groups.
Conclusion(s): Using high sensitivity methods, we detected the presence of bacteria in a subset of CSF samples at the time of first surgery. Therefore, the true presence of bacteria in CSF of children with hydrocephalus cannot be ruled out, though our findings may suggest these bacteria are contaminants or false positives of the detection methods. Regardless of origin, the detection of microbiota in the CSF of these children may not have any clinical significance.
Copyright: © 2023 Pandey et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
