

Long-term Outcomes in Primary CNS Lymphoma After R-MVP and High-Dose Chemotherapy With Autologous Hematopoietic Stem Cell Transplant
- PMID: 37344228
- PMCID: PMC10437028
- DOI: 10.1212/WNL.0000000000207490
Long-term Outcomes in Primary CNS Lymphoma After R-MVP and High-Dose Chemotherapy With Autologous Hematopoietic Stem Cell Transplant
Abstract
Background and objectives: Primary CNS lymphoma (PCNSL), a rare CNS malignancy, is usually treated with high-dose methotrexate in the first-line setting, typically followed by consolidation therapy. Due to the broad range of currently available treatments for PCNSL, comparability in long-term follow-up studies is limited, and data are scattered across small studies.
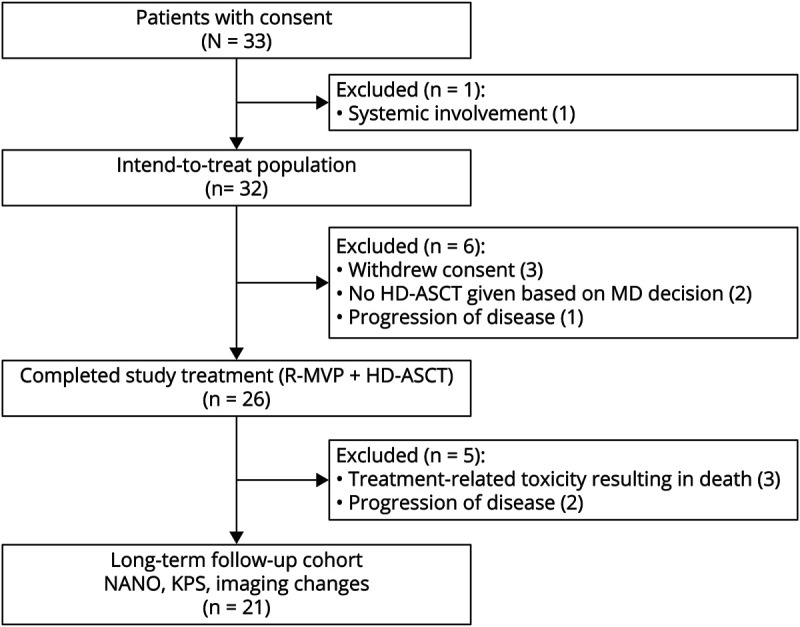
Methods: In this study, we report the long-term survival of patients with newly diagnosed immunocompetent PCNSL, enrolled in a phase II trial from June 2005 to September 2011. Patients were treated using rituximab, methotrexate, vincristine, and procarbazine (R-MVP) chemotherapy followed by high-dose chemotherapy (HDC) and autologous stem cell transplant (ASCT) in those with partial or complete response to R-MVP. In a post hoc analysis, clinical and imaging features were evaluated in those still alive.
Results: 26 of 32 patients underwent HDC-ASCT consolidation. Of them, 3 patients died of treatment-related toxicity and 2 due to disease progression within 1 year of ASCT. None of the remaining 21 patients had disease progression with a median follow-up of 12.1 years and were included in the analysis. Compared with the post-HDC-ASCT assessment, at the last follow-up, there was no significant difference in the median Karnofsky Performance Status (80 [range: 60-100] vs 90 [range: 70-100]), the median Neurologic Assessment in Neuro-Oncology score (1 [range: 0-4] vs 1 [range: 0-5]), and leukoencephalopathy score (1 [range: 0-3] vs 1 [range: 1-4]).
Discussion: Long-term follow-up demonstrated that treatment was well tolerated in most patients enrolled in this study, with stable leukoencephalopathy on imaging and stable clinical performance status. Disease recurrence was not observed beyond 2 years after HDC-ASCT consolidation.
© 2023 American Academy of Neurology.
Conflict of interest statement
The authors report no relevant disclosures. Go to
Figures



References
-
- Jahnke K, Thiel E, Martus P, et al. . Relapse of primary central nervous system lymphoma: clinical features, outcome and prognostic factors. J Neurooncol. 2006;80(2):159-165. - PubMed
-
- Gavrilovic IT, Hormigo A, Yahalom J, Deangelis LM, Abrey LE. Long-term follow-up of high-dose methotrexate-based therapy with and without whole brain irradiation for newly diagnosed primary CNS lymphoma. J Clin Oncol. 2006;24(28):4570-4574. - PubMed
-
- Houillier C, Taillandier L, Dureau S, et al. . Radiotherapy or autologous stem-cell transplantation for primary CNS lymphoma in patients 60 years of age and younger: results of the intergroup ANOCEF-GOELAMS randomized phase II PRECIS study. J Clin Oncol. 2019;37(10):823-833. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous