

Long-term Multidomain Patterns of Change After Traumatic Brain Injury: A TRACK-TBI LONG Study
- PMID: 37344231
- PMCID: PMC10437015
- DOI: 10.1212/WNL.0000000000207501
Long-term Multidomain Patterns of Change After Traumatic Brain Injury: A TRACK-TBI LONG Study
Abstract
Background and objectives: Traumatic brain injury (TBI) may be a chronic condition carrying risk of future sequelae; few prospective studies examine long-term postinjury outcomes. We examined the prevalence of functional, cognitive, and psychiatric change outcomes from 1 to 7 years postinjury.
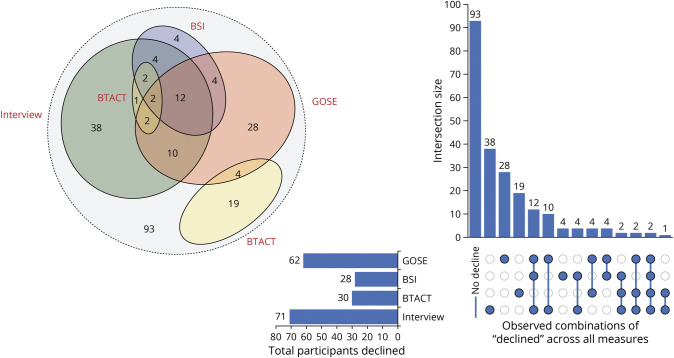
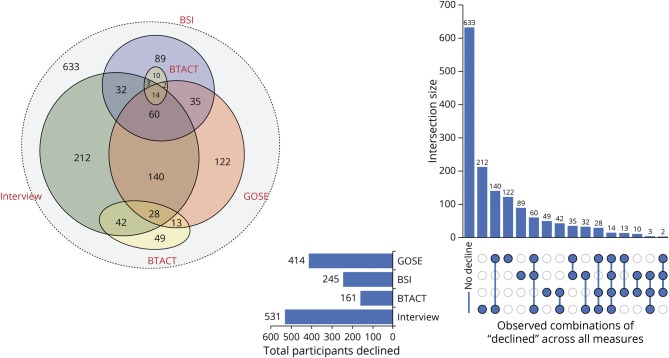
Methods: Transforming Research and Clinical Knowledge in TBI LONG (TRACK-TBI LONG) participants were prospectively enrolled within 24 hours of injury and followed up to 1 year postinjury; a subset participated in long-term follow-up from 2 to 7 years postinjury. Reliable change thresholds for the Brief Test of Adult Cognition by Telephone General Composite (cognition) and Brief Symptom Inventory (BSI)-18 (psychiatric) were derived from orthopedic trauma controls (OTCs). Multiple assessments were completed (postinjury baseline assessment and 2 or 3 visits 2-7 years postinjury) within a sample subset. Change was assessed for functional outcome (Glasgow Outcome Scale-Extended [GOSE]) and self-report/informant report of decline. Prevalence ratios for outcomes classified as stable, improved, and declined were reported individually and collectively. The Fisher exact test and log-binomial regression models examined factors associated with decline and improvement.
Results: Of the sample (N = 1,264; mild TBI [mTBI], Glasgow Coma Scale [GCS] 13-15, n = 917; moderate-to-severe TBI [msTBI], GCS 3-12, n = 193; or OTC n = 154), "stable" was the most prevalent outcome. Functional outcome showed the highest rates of decline, regardless of TBI severity (mild = 29%; moderate/severe = 23%). When measures were collectively considered, rates of decline included mTBI (21%), msTBI (26%), and OTC (15%). Age and preinjury employment status were associated with functional decline (per 10 years; relative risk [RR] 1.16, 95% CI 1.07-1.25, p < 0.001; higher in retired/disabled/not working vs full-time/part-time; RR 1.81, 95% CI 1.33-2.45, respectively) in the mTBI group. Improvement in functional recovery 2-7 years postinjury was associated with higher BSI scores (per 5 points; RR 1.11, 95% CI 1.04-1.18, p = 0.002) and GOSE score of 5-7 (GOSE = 8 as reference; RR 2.64, 95% CI 1.75-3.97, p < 0.001). Higher BSI scores and identifying as Black (RR 2.28, 95% CI 1.59-3.25, p < 0.001) were associated with a greater likelihood of improved psychiatric symptoms in mTBI (RR 1.21, 95% CI 1.14-1.29, p < 0.001). A greater likelihood of cognitive improvement was observed among those with higher educational attainment in msTBI (per 4 years; RR 2.61, 95% CI 1.43-4.79, p = 0.002).
Discussion: Function across domains at 1-year postinjury, a common recovery benchmark, undergoes change across the subsequent 6 years. Results support consideration of TBI as a chronic evolving condition and suggest continued monitoring, rehabilitation, and support is required to optimize long-term independence and quality of life.
© 2023 American Academy of Neurology.
Conflict of interest statement
B.L. Brett reports grants from the National Institute on Aging and National Institute of Neurological Disorders and Stroke (NINDS). N. Temkin reported receiving grants from the US Department of Defense (DoD) and NIH/NINDS during the conduct of the study. M. Stein reported receiving grants from the NIH subcontract from University of California, San Francisco (UCSF) during the conduct of the study; other from Oxeia Biopharmaceuticals Stock options outside the submitted work. J.T. Giacino reported receiving support from the UCSF subcontract during the conduct of the study. M.A. McCrea reported receiving grants from the UCSF, Research subaward to Medical College of Wisconsin during the conduct of the study. Y.G. Bodien reported receiving grants from NINDS, DoD, James S. McDonnell Foundation, Tiny Blue Dot, and National Institute on Disability, Independent Living, and Rehabilitation Research during the conduct of the study. J. Corrigan reported receiving grants from the NIH during the conduct of the study. R. Diaz-Arrastia reported receiving grants from the NIH and DoD during the conduct of the study; owing stock in BrainBox and Nia Therapeutics; and personal fees from Pinteon Therapeutics, MesoScale Discoveries, and Ischemix outside the submitted work. L. Nelson reported receiving grants from the NINDS, Centers for Disease Control and Prevention, DoD, and Advancing a Healthier Wisconsin outside the submitted work. Go to
Figures
Comment in
-
Clinical outcomes evolve years after traumatic brain injury.Nat Rev Neurol. 2023 Oct;19(10):579-580. doi: 10.1038/s41582-023-00868-1. Nat Rev Neurol. 2023. PMID: 37700090 No abstract available.