

Obesity paradox as a new insight from postoperative complications in gastric cancer
- PMID: 37344511
- PMCID: PMC10284837
- DOI: 10.1038/s41598-023-36968-7
Obesity paradox as a new insight from postoperative complications in gastric cancer
Abstract
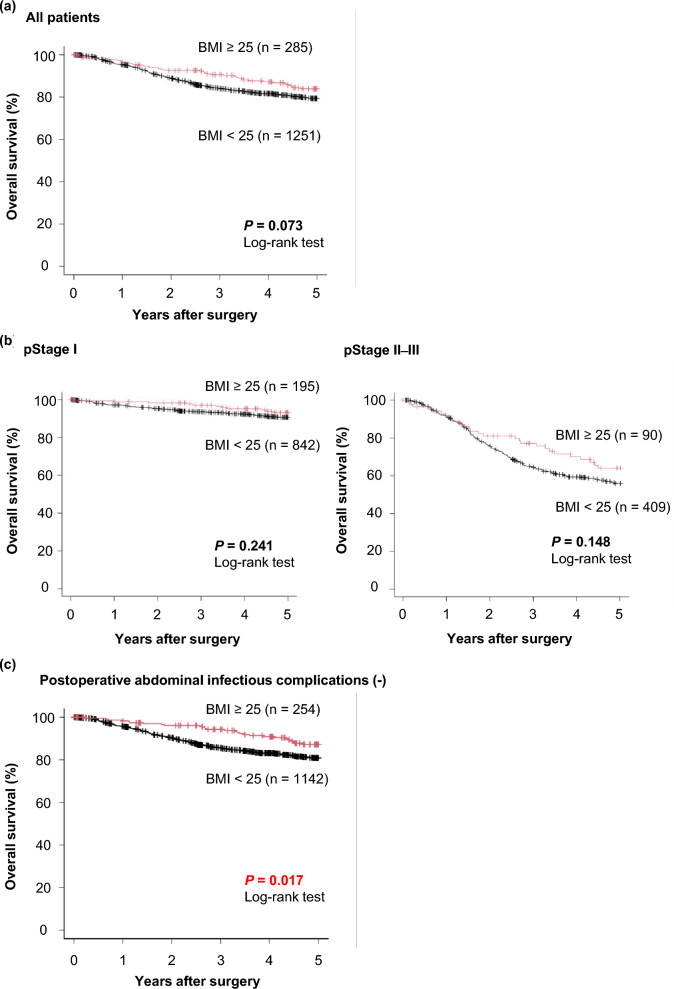
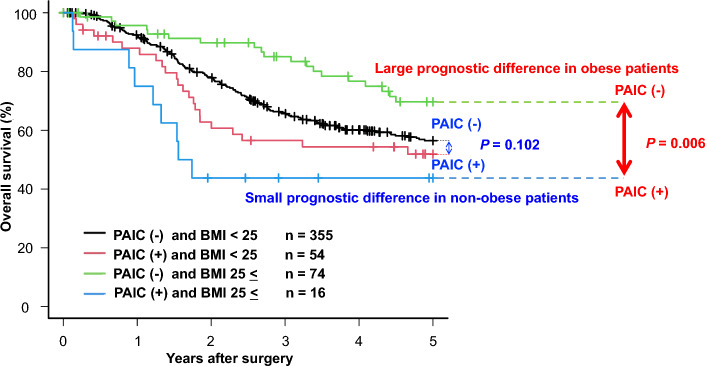
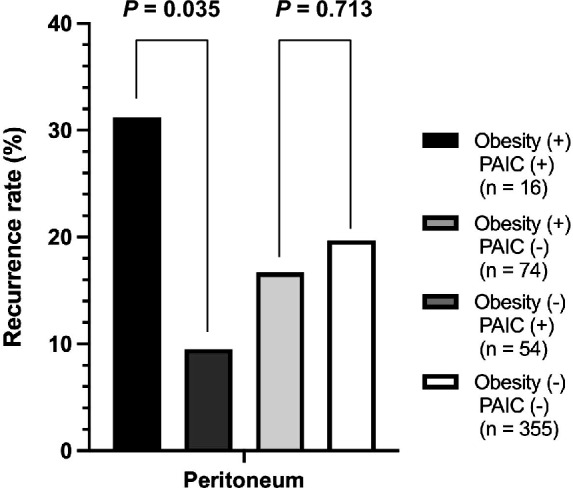
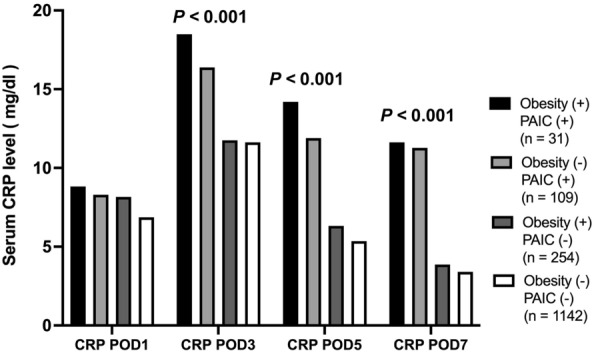
The obesity paradox is reported to exist in various diseases. However, obesity is a pivotal issue in gastric cancer (GC) patients because of the surgical difficulty related to postoperative abdominal infectious complications (PAIC). This study clarified the existence of the obesity paradox in GC. Between 1997 and 2015, 1536 consecutive patients underwent curative gastrectomy. Of all patients, 18.6% (285/1536) were obese and tended to have a better prognosis (P = 0.073). In patients without PAIC, obesity was a significant prognostic factor for 5-year overall survival (P = 0.017). PAIC was an independent poor prognostic factor in both obese and non-obese patients (P < 0.001; hazard ratio [HR] 4.22 and 1.82). In pStage II-III patients, there was a large and significant prognostic difference between non-PAIC and PAIC obese patients (P = 0.006; 5-year overall survival: 69.7% vs. 43.8%) related to the higher incidence of peritoneal recurrence in PAIC obese patients (P = 0.035; 31% vs. 10%). Whereas, there was a small prognostic difference between non-PAIC and PAIC non-obese patients (P = 0.102; 5-year overall survival: 56.5% vs. 51.9%). Although the obesity paradox is present in GC, PAIC had a more negative prognostic impact through peritoneal recurrence in obese GC patients.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Prognostic analysis of patients with intra-abdominal infectious complications after laparoscopic-assisted and open radical gastrectomy for gastric cancer - A propensity score-matching analysis.Surg Oncol. 2021 Jun;37:101583. doi: 10.1016/j.suronc.2021.101583. Epub 2021 May 14. Surg Oncol. 2021. PMID: 34087739
-
Prognostic impact of infectious complications after curative gastric cancer surgery.Eur J Surg Oncol. 2020 Jul;46(7):1233-1238. doi: 10.1016/j.ejso.2020.04.032. Epub 2020 Apr 23. Eur J Surg Oncol. 2020. PMID: 32362466
-
Non-robotic minimally invasive gastrectomy as an independent risk factor for postoperative intra-abdominal infectious complications: A single-center, retrospective and propensity score-matched analysis.World J Gastroenterol. 2020 Mar 21;26(11):1172-1184. doi: 10.3748/wjg.v26.i11.1172. World J Gastroenterol. 2020. PMID: 32231421 Free PMC article.
-
Postoperative complications and prognosis after radical gastrectomy for gastric cancer: a systematic review and meta-analysis of observational studies.World J Surg Oncol. 2019 Mar 18;17(1):52. doi: 10.1186/s12957-019-1593-9. World J Surg Oncol. 2019. PMID: 30885211 Free PMC article.
-
Relationship Between Postoperative Complications and the Prognosis of Gastric Carcinoma Patients Who Underwent Surgical Resection: A Systematic Review and Meta-Analysis.Cancer Control. 2021 Jan-Dec;28:10732748211011955. doi: 10.1177/10732748211011955. Cancer Control. 2021. PMID: 34018400 Free PMC article.
Cited by
-
Adipose Tissue Quantification Improves the Prognostic Value of GLIM Criteria in Advanced Gastric Cancer Patients.Nutrients. 2024 Mar 2;16(5):728. doi: 10.3390/nu16050728. Nutrients. 2024. PMID: 38474856 Free PMC article.
-
The multifactorial effect of obesity on the effectiveness and outcomes of cancer therapies.Nat Rev Endocrinol. 2024 Dec;20(12):701-714. doi: 10.1038/s41574-024-01032-5. Epub 2024 Sep 23. Nat Rev Endocrinol. 2024. PMID: 39313571 Review.
References
-
- The Foundation for Promotion of Cancer Research (FPCR). Cancer Statistics in JAPAN 2018. (2018).
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
