

Exploring variation in implementation of multifactorial falls risk assessment and tailored interventions: a realist review
- PMID: 37344760
- PMCID: PMC10286425
- DOI: 10.1186/s12877-023-04045-3
Exploring variation in implementation of multifactorial falls risk assessment and tailored interventions: a realist review
Abstract
Background: Falls are the most common safety incident reported by acute hospitals. In England national guidance recommends delivery of a multifactorial falls risk assessment (MFRA) and interventions tailored to address individual falls risk factors. However, there is variation in how these practices are implemented. This study aimed to explore the variation by examining what supports or constrains delivery of MFRAs and tailored interventions in acute hospitals.
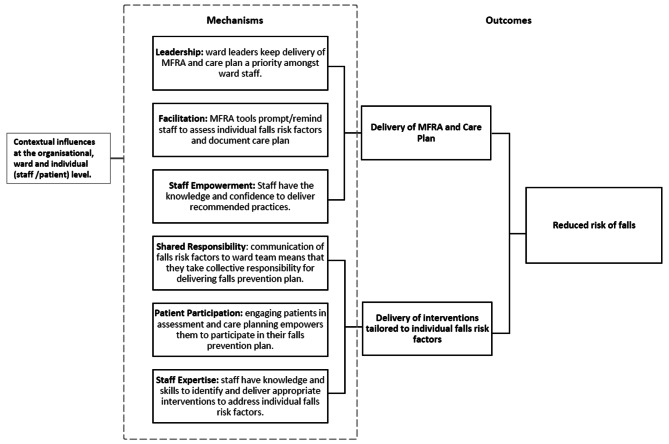
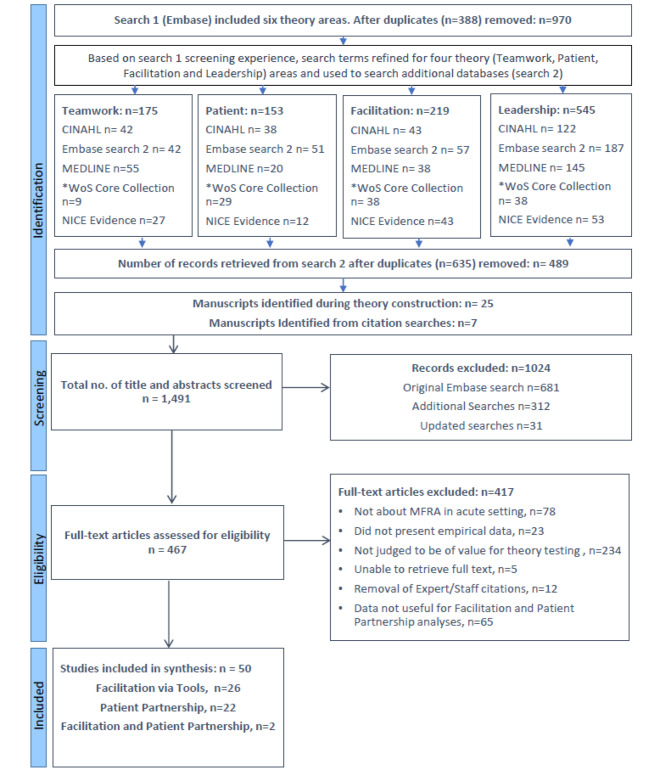
Methods: A realist review of literature was conducted with searches completed in three stages: (1) to construct hypotheses in the form of Context, Mechanism, Outcome configurations (CMOc) about how MFRAs and interventions are delivered, (2) to scope the breadth and depth of evidence available in Embase to test the CMOcs, and (3) following prioritisation of CMOcs, to refine search strategies for use in multiple databases. Citations were managed in EndNote; titles, abstracts, and full texts were screened, with 10% independently screened by two reviewers.
Results: Two CMOcs were prioritised for testing labelled: Facilitation via MFRA tools, and Patient Participation in interventions. Analysis indicated that MFRA tools can prompt action, but the number and type of falls risk factors included in tools differ across organisations leading to variation in practice. Furthermore, the extent to which tools work as prompts is influenced by complex ward conditions such as changes in patient condition, bed swaps, and availability of falls prevention interventions. Patient participation in falls prevention interventions is more likely where patient directed messaging takes individual circumstances into account, e.g., not wanting to disturb nurses by using the call bell. However, interactions that elicit individual circumstances can be resource intensive and patients with cognitive impairment may not be able to participate despite appropriately directed messaging.
Conclusions: Organisations should consider how tools can be developed in ways that better support consistent and comprehensive identification of patients' individual falls risk factors and the complex ward conditions that can disrupt how tools work as facilitators. Ward staff should be supported to deliver patient directed messaging that is informed by their individual circumstances to encourage participation in falls prevention interventions, where appropriate.
Trial registration: PROSPERO: CRD42020184458.
Keywords: Falls; Falls prevention; Patient participation; Realist review; Risk assessment.
© 2023. The Author(s).
Conflict of interest statement
I declare that the authors have no competing interests as defined by BMC, or other interests that might be perceived to influence the results and/or discussion reported in this paper.
Figures
References
-
- NHS Improvement . The incidence and costs of inpatient falls in hospitals. London: NHS Improvement; 2017.
-
- Oliver D. Preventing falls and fall injuries in hospital: a major risk management challenge. Clin Risk. 2007;13(5):173–8. doi: 10.1258/135626207781572693. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
