

Effectiveness of interventions by non-professional community-level workers or family caregivers to improve outcomes for physical impairments or disabilities in low resource settings: systematic review of task-sharing strategies
- PMID: 37344907
- PMCID: PMC10286375
- DOI: 10.1186/s12960-023-00831-7
Effectiveness of interventions by non-professional community-level workers or family caregivers to improve outcomes for physical impairments or disabilities in low resource settings: systematic review of task-sharing strategies
Abstract
Background: In low-resource settings, access to basic rehabilitation could be supplemented by community-level interventions provided by community health workers, health volunteers, or family caregivers. Yet, it is unclear whether basic physical rehabilitation interventions delivered to adults by non-professional alternative resources in the community, under task-shifting or task-sharing approaches, are effective as those delivered by skilled rehabilitation professionals. We aim to synthesize evidence on the effectiveness of community-level rehabilitation interventions delivered by non-professional community-level workers or informal caregivers to improve health outcomes for persons with physical impairments or disabilities.
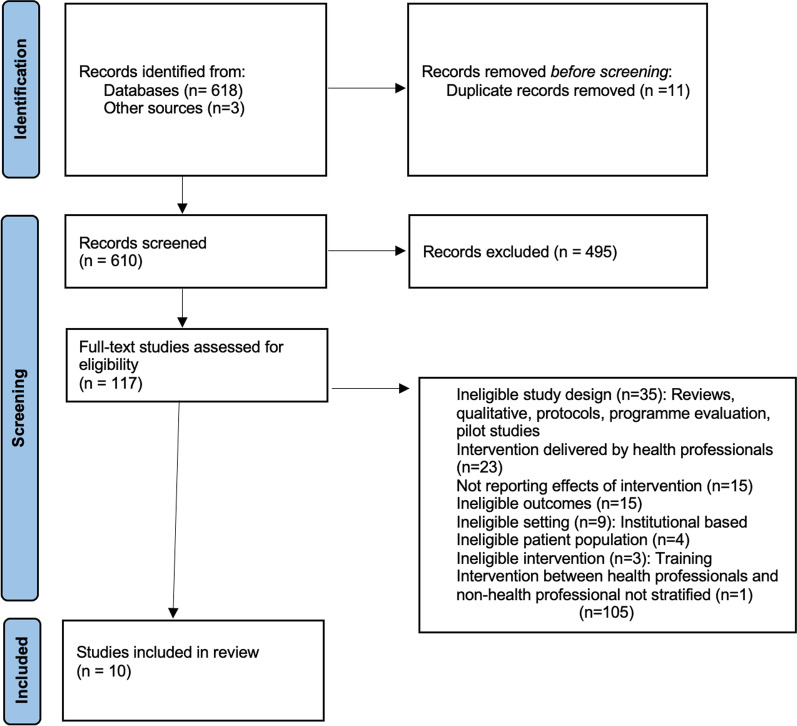
Methods: We performed a systematic review with a PROSPERO registration. Eight databases were searched for (PubMed, CINAHL, Global Health, PDQ Evidence, Scopus, ProQuest, CENTRAL, and Web of Science), supplemented by snowballing and key-informant recommendations, with no time restrictions, applied. Controlled and non-controlled experiments were included if reporting the effects of interventions on mobility, activities of daily living (ADLs), quality of life, or social participation outcomes. Two independent investigators performed the eligibility decisions, data extraction, risk of bias, and assessed the quality of the evidence using the GRADE approach.
Results: Ten studies (five randomized controlled trials [RCTs]) involving 2149 participants were included. Most common targeted stroke survivors (n = 8); family caregivers were most frequently used to deliver the intervention (n = 4); and the intervention was usually provided in homes (n = 7), with training initiated in the hospital (n = 4). Of the four RCTs delivered by family caregivers, one demonstrated a statistically significant improvement in mobility (effect size: 0.3; confidence interval [CI] 121.81-122.19; [p = 0.04]) and another one in ADLs (effect size: 0.4; CI 25.92-35.08; [p = 0.03]). Of the five non-RCT studies by community health workers or volunteers, one demonstrated a statistically significant improvement in mobility (effect size: 0.3; CI 10.143-16.857; [p < 0.05]), while two demonstrated improved statistically significant improvement in ADLs (effect size: 0.2; CI 180.202-184.789 [p = 0.001]; 0.4; CI - 7.643-18.643; [p = 0.026]). However, the quality of evidence, based on GRADE criteria, was rated as low to very low.
Conclusions: While task-sharing is a possible strategy to meet basic rehabilitation needs in low-resource settings, the current evidence on the effectiveness of delivering rehabilitation interventions by non-professional community-level workers and informal caregivers is inconclusive. We can use the data and experiences from existing studies to better design studies and improve the implementation of interventions. Trial registration PROSPERO registration number: CRD42022319130.
Keywords: Adults; Community health workers; Family caregivers; Health volunteers; Low-resource settings; Non-healthcare providers; Physical disabilities; Physical function; Systematic review.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Interventions for preventing abuse in the elderly.Cochrane Database Syst Rev. 2016 Aug 16;2016(8):CD010321. doi: 10.1002/14651858.CD010321.pub2. Cochrane Database Syst Rev. 2016. PMID: 27528431 Free PMC article.
-
Technological aids for the rehabilitation of memory and executive functioning in children and adolescents with acquired brain injury.Cochrane Database Syst Rev. 2016 Jul 1;7(7):CD011020. doi: 10.1002/14651858.CD011020.pub2. Cochrane Database Syst Rev. 2016. PMID: 27364851 Free PMC article.
-
Caregiver-mediated exercises for improving outcomes after stroke.Cochrane Database Syst Rev. 2016 Dec 21;12(12):CD011058. doi: 10.1002/14651858.CD011058.pub2. Cochrane Database Syst Rev. 2016. PMID: 28002636 Free PMC article.
-
Interventions to improve hearing aid use in adult auditory rehabilitation.Cochrane Database Syst Rev. 2016 Aug 18;2016(8):CD010342. doi: 10.1002/14651858.CD010342.pub3. Cochrane Database Syst Rev. 2016. PMID: 27537242 Free PMC article.
-
Yoga for stroke rehabilitation.Cochrane Database Syst Rev. 2017 Dec 8;12(12):CD011483. doi: 10.1002/14651858.CD011483.pub2. Cochrane Database Syst Rev. 2017. PMID: 29220541 Free PMC article.
Cited by
-
Practical insights for enhancing primary care rehabilitation services in low-resource contexts.Afr J Prim Health Care Fam Med. 2025 Feb 6;17(1):e1-e13. doi: 10.4102/phcfm.v17i1.4699. Afr J Prim Health Care Fam Med. 2025. PMID: 39935123 Free PMC article.
-
Education of Occupational Therapists in Mental Health: A Global Survey of Educators Regarding Perceived Facilitators and Barriers.Int J Environ Res Public Health. 2025 Jun 26;22(7):1009. doi: 10.3390/ijerph22071009. Int J Environ Res Public Health. 2025. PMID: 40724076 Free PMC article.
-
A qualitative study on rehabilitation services at primary health care: insights from primary health care stakeholders in low-resource contexts.BMC Health Serv Res. 2024 Oct 23;24(1):1272. doi: 10.1186/s12913-024-11748-9. BMC Health Serv Res. 2024. PMID: 39438887 Free PMC article.
-
The influence of contextual factors on an intervention for people with disabilities from support persons' and health personnel's perspectives: a focus group study.Front Rehabil Sci. 2024 May 1;5:1294990. doi: 10.3389/fresc.2024.1294990. eCollection 2024. Front Rehabil Sci. 2024. PMID: 38751820 Free PMC article.
References
-
- WHO. Chapter 4 rehabilitation. World report on disability. 2006.
-
- WHO. World report on disability. 2011.
-
- WHO. The need to scale up rehabilitation. Rehabilitation. 2017. p. 1–9. https://www.who.int/disabilities/care/NeedToScaleUpRehab.pdf; http://www.who.int/disabilities/care/Need-to-scale-up-rehab-July2018.pdf....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
