

Novel Targets, Novel Treatments: The Changing Landscape of Non-Small Cell Lung Cancer
- PMID: 37345192
- PMCID: PMC10216085
- DOI: 10.3390/cancers15102855
Novel Targets, Novel Treatments: The Changing Landscape of Non-Small Cell Lung Cancer
Abstract
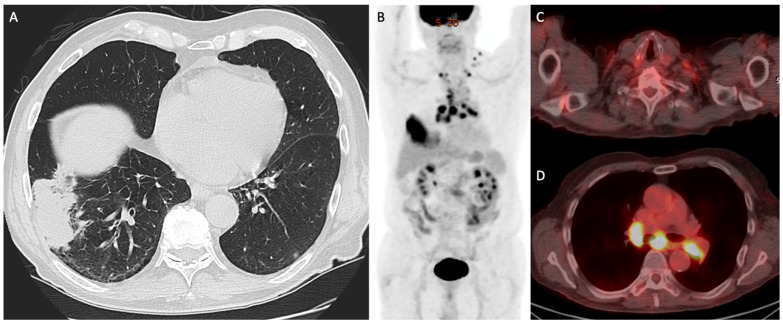
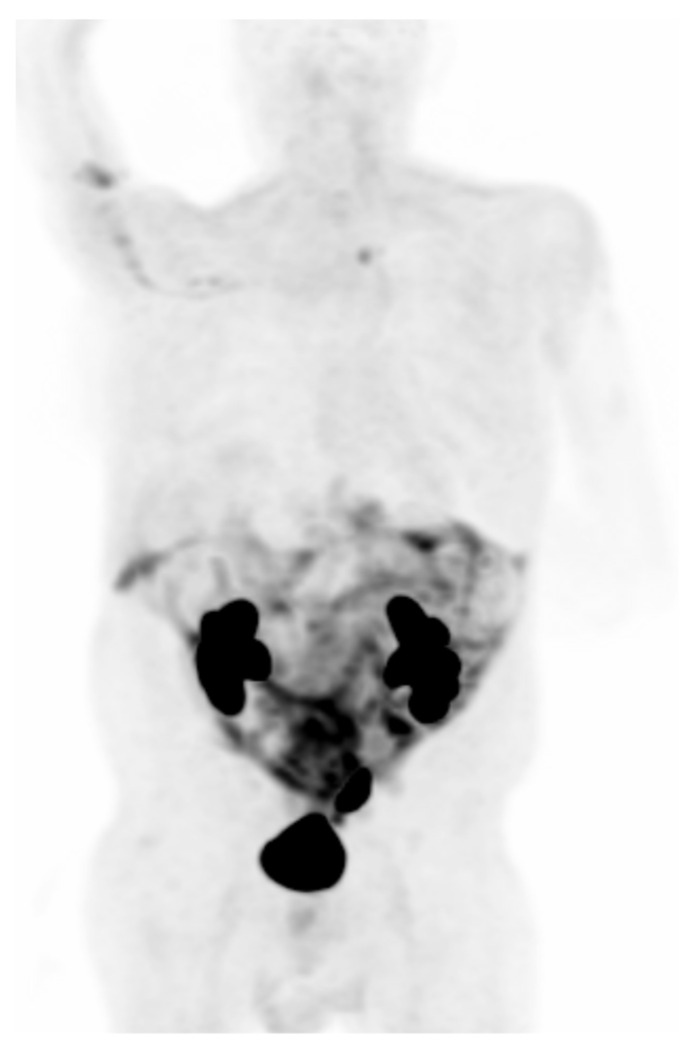
Treatment of non-small cell lung cancer (NSCLC) has undergone a paradigm shift. Once a disease with limited potential therapies, treatment options for patients have exploded with the availability of molecular testing to direct management and targeted therapies to treat tumors with specific driver mutations. New in vitro diagnostics allow for the early and non-invasive detection of disease, and emerging in vivo imaging techniques allow for better detection and monitoring. The development of checkpoint inhibitor immunotherapy has arguably been the biggest advance in lung cancer treatment, given that the vast majority of NSCLC tumors can be treated with these therapies. Specific targeted therapies, including those against KRAS, EGFR, RTK, and others have also improved the outcomes for those individuals bearing an actionable mutation. New and emerging therapies, such as bispecific antibodies, CAR T cell therapy, and molecular targeted radiotherapy, offer promise to patients for whom none of the existing therapies have proved effective. In this review, we provide the most up-to-date survey to our knowledge regarding emerging diagnostic and therapeutic strategies for lung cancer to provide clinicians with a comprehensive reference of the options for treatment available now and those which are soon to come.
Keywords: PET imaging; lung cancer; molecular diagnostics; targeted therapies.
Conflict of interest statement
Salvatore is a speaker and consultant for Genentech and Boehringer Ingelheim and has received grant funding from Genentech and Boehringer Ingelheim. Capaccione has served as an advisor for Cardinal Health. The remaining authors have nothing to disclose. No funding was obtained for this study.
Figures




References
-
- Howington J.A., Blum M.G., Chang A.C., Balekian A.A., Murthy S.C. Treatment of stage I and II non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143:e278S–e313S. doi: 10.1378/chest.12-2359. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
