

Metabolic Signatures of Cardiac Dysfunction, Multimorbidity, and Post-Transcatheter Aortic Valve Implantation Death
- PMID: 37345820
- PMCID: PMC10356077
- DOI: 10.1161/JAHA.123.029542
Metabolic Signatures of Cardiac Dysfunction, Multimorbidity, and Post-Transcatheter Aortic Valve Implantation Death
Abstract
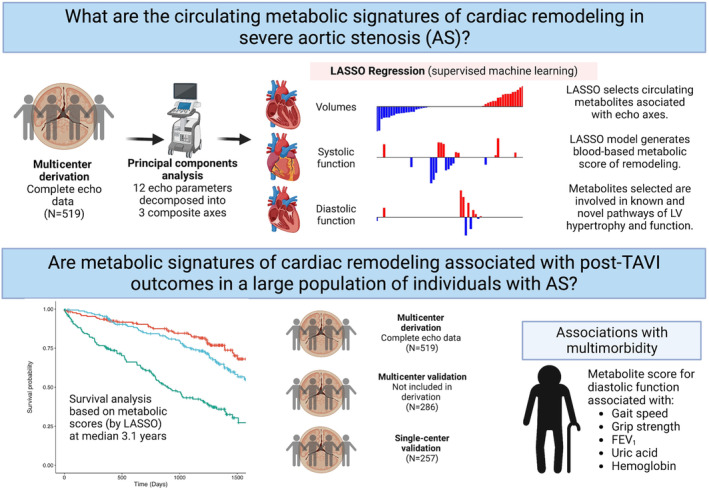
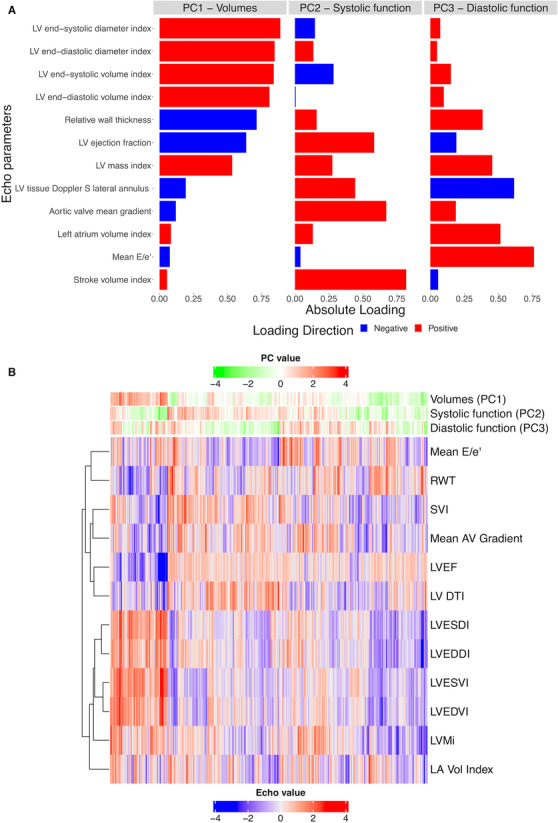
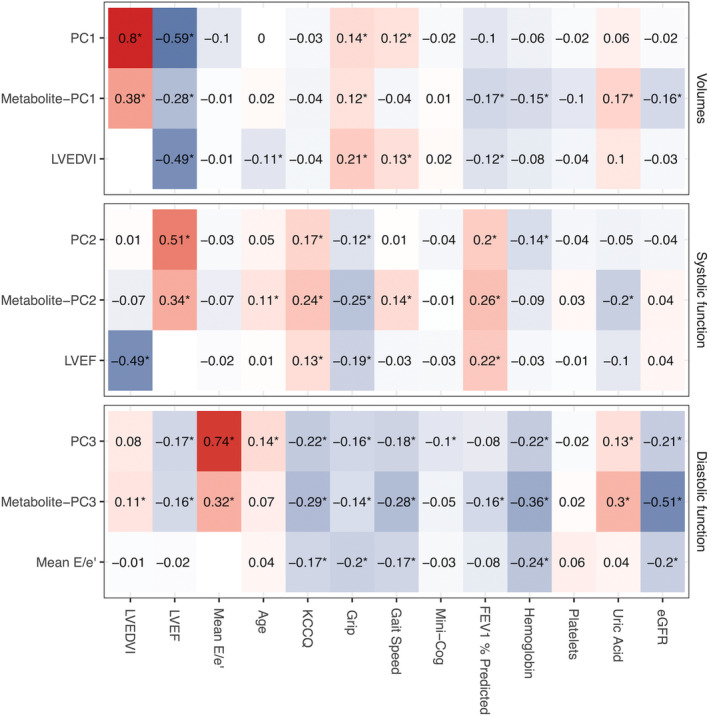
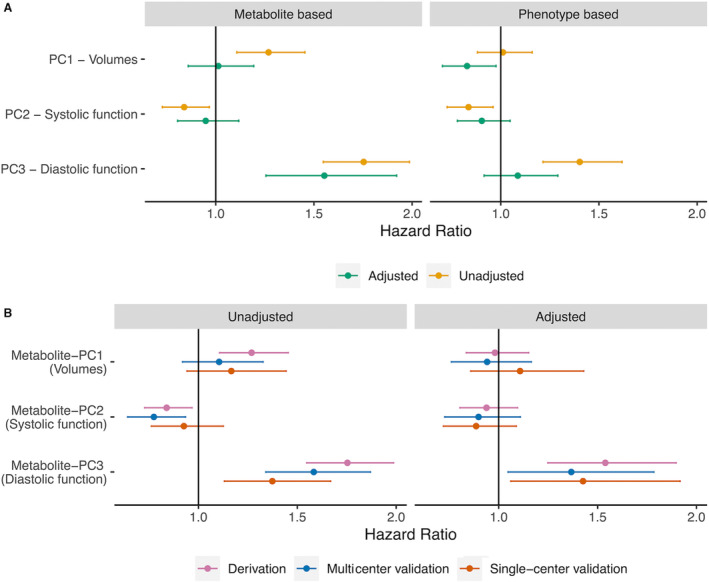
Background Studies in mice and small patient subsets implicate metabolic dysfunction in cardiac remodeling in aortic stenosis, but no large comprehensive studies of human metabolism in aortic stenosis with long-term follow-up and characterization currently exist. Methods and Results Within a multicenter prospective cohort study, we used principal components analysis to summarize 12 echocardiographic measures of left ventricular structure and function pre-transcatheter aortic valve implantation in 519 subjects (derivation). We used least absolute shrinkage and selection operator regression across 221 metabolites to define metabolic signatures for each structural pattern and measured their relation to death and multimorbidity in the original cohort and up to 2 validation cohorts (N=543 for overall validation). In the derivation cohort (519 individuals; median age, 84 years, 45% women, 95% White individuals), we identified 3 axes of left ventricular remodeling, broadly specifying systolic function, diastolic function, and chamber volumes. Metabolite signatures of each axis specified both known and novel pathways in hypertrophy and cardiac dysfunction. Over a median of 3.1 years (205 deaths), a metabolite score for diastolic function was independently associated with post-transcatheter aortic valve implantation death (adjusted hazard ratio per 1 SD increase in score, 1.54 [95% CI, 1.25-1.90]; P<0.001), with similar effects in each validation cohort. This metabolite score of diastolic function was simultaneously associated with measures of multimorbidity, suggesting a metabolic link between cardiac and noncardiac state in aortic stenosis. Conclusions Metabolite profiles of cardiac structure identify individuals at high risk for death following transcatheter aortic valve implantation and concurrent multimorbidity. These results call for efforts to address potentially reversible metabolic biology associated with risk to optimize post-transcatheter aortic valve implantation recovery, rehabilitation, and survival.
Keywords: aortic stenosis; metabolomics; outcomes; remodeling.
Figures
References
-
- Arnold SV, Cohen DJ, Dai D, Jones PG, Li F, Thomas L, Baron SJ, Frankel NZ, Strong S, Matsouaka RA, et al. Predicting quality of life at 1 year after transcatheter aortic valve replacement in a real‐world population. Circ Cardiovasc Qual Outcomes. 2018;11:e004693. doi: 10.1161/CIRCOUTCOMES.118.004693 - DOI - PMC - PubMed
-
- Hermiller JB Jr, Yakubov SJ, Reardon MJ, Deeb GM, Adams DH, Afilalo J, Huang J, Popma JJ; CoreValve United States Clinical Investigators . Predicting early and late mortality after transcatheter aortic valve replacement. J Am Coll Cardiol. 2016;68:343–352. doi: 10.1016/j.jacc.2016.04.057 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
