

Safety and effectiveness of vonoprazan-based rescue therapy for Helicobacter pylori infection
- PMID: 37346155
- PMCID: PMC10280792
- DOI: 10.3748/wjg.v29.i20.3133
Safety and effectiveness of vonoprazan-based rescue therapy for Helicobacter pylori infection
Abstract
Background: Vonoprazan (VPZ)-based regimens are an effective first-line therapy for Helicobacter pylori (H. pylori) infection. However, their value as a rescue therapy needs to be explored.
Aim: To assess a VPZ-based regimen as H. pylori rescue therapy.
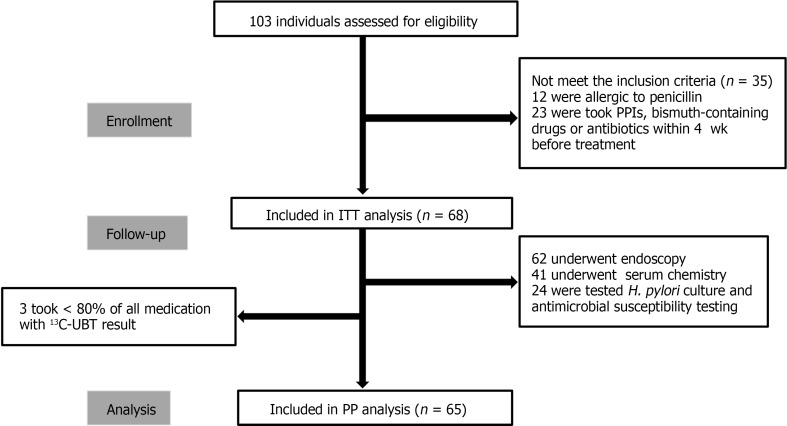
Methods: This prospective, single-center, clinical trial was conducted between January and August 2022. Patients with a history of H. pylori treatment failure were administered 20 mg VPZ twice daily, 750 mg amoxicillin 3 times daily, and 250 mg Saccharomyces boulardii (S. boulardii) twice daily for 14 d (14-d VAS regimen). VPZ and S. boulardii were taken before meals, while amoxicillin was taken after meals. Within 3 d after the end of eradication therapy, all patients were asked to fill in a questionnaire to assess any adverse events they may have experienced. At least 4-6 wk after the end of eradication therapy, eradication success was assessed using a 13C-urea breath test, and factors associated with eradication success were explored.
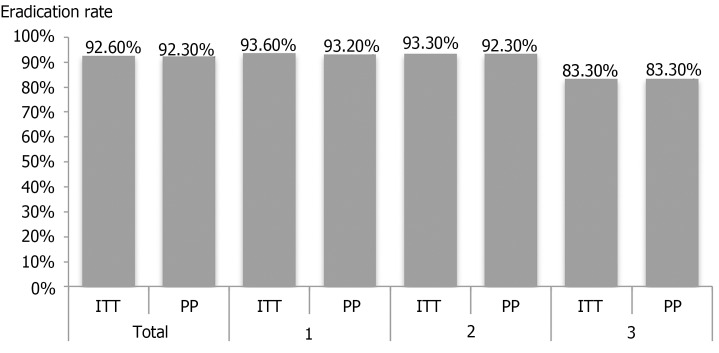
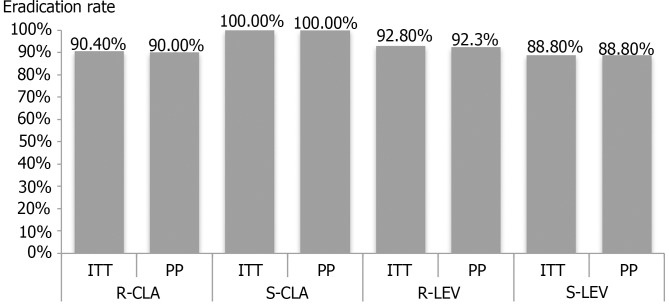
Results: Herein, 103 patients were assessed, and 68 patients were finally included. All included patients had 1-3 previous eradication failures. The overall eradication rates calculated using intention-to-treat and per-protocol analyses were 92.6% (63/68) and 92.3% (60/65), respectively. The eradication rate did not differ with the number of treatment failures (P = 0.433). The rates of clarithromycin, metronidazole, and levofloxacin resistance were 91.3% (21/23), 100.0% (23/23), and 60.9% (14/23), respectively. There were no cases of resistance to tetracycline, amoxicillin, or furazolidone. In 60.9% (14/23) patients, the H. pylori isolate was resistant to all 3 antibiotics (clarithromycin, metronidazole, and levofloxacin); however, eradication was achieved in 92.9% (13/14) patients. All patients showed metronidazole resistance, and had an eradication rate of 91.3% (21/23). The eradication rate was higher among patients without anxiety (96.8%) than among patients with anxiety (60.0%, P = 0.025). No severe adverse events occurred; most adverse events were mild and disappeared without intervention. Good compliance was seen in 95.6% (65/68) patients. Serological examination showed no significant changes in liver and kidney function.
Conclusion: VAS is a safe and effective rescue therapy, with an acceptable eradication rate (> 90%), regardless of the number of prior treatment failures. Anxiety may be associated with eradication failure.
Keywords: Helicobacter pylori; Anxiety; Eradication; Rescue therapy; Saccharomyces boulardii; Vonoprazan.
©The Author(s) 2023. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflict of interest.
Figures
References
-
- Zamani M, Ebrahimtabar F, Zamani V, Miller WH, Alizadeh-Navaei R, Shokri-Shirvani J, Derakhshan MH. Systematic review with meta-analysis: the worldwide prevalence of Helicobacter pylori infection. Aliment Pharmacol Ther. 2018;47:868–876. - PubMed
-
- Chiang TH, Chang WJ, Chen SL, Yen AM, Fann JC, Chiu SY, Chen YR, Chuang SL, Shieh CF, Liu CY, Chiu HM, Chiang H, Shun CT, Lin MW, Wu MS, Lin JT, Chan CC, Graham DY, Chen HH, Lee YC. Mass eradication of Helicobacter pylori to reduce gastric cancer incidence and mortality: a long-term cohort study on Matsu Islands. Gut. 2021;70:243–250. - PMC - PubMed
-
- Liu WZ, Xie Y, Lu H, Cheng H, Zeng ZR, Zhou LY, Chen Y, Wang JB, Du YQ, Lu NH Chinese Society of Gastroenterology, Chinese Study Group on Helicobacter pylori and Peptic Ulcer. Fifth Chinese National Consensus Report on the management of Helicobacter pylori infection. Helicobacter. 2018;23:e12475. - PubMed
-
- Chey WD, Leontiadis GI, Howden CW, Moss SF. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am J Gastroenterol. 2017;112:212–239. - PubMed
-
- Malfertheiner P, Megraud F, Rokkas T, Gisbert JP, Liou JM, Schulz C, Gasbarrini A, Hunt RH, Leja M, O’Morain C, Rugge M, Suerbaum S, Tilg H, Sugano K, El-Omar EM European Helicobacter and Microbiota Study group. Management of Helicobacter pylori infection: the Maastricht VI/Florence consensus report. Gut. 2022
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
