

Medicinal cannabis for psychiatry-related conditions: an overview of current Australian prescribing
- PMID: 37346297
- PMCID: PMC10279775
- DOI: 10.3389/fphar.2023.1142680
Medicinal cannabis for psychiatry-related conditions: an overview of current Australian prescribing
Abstract
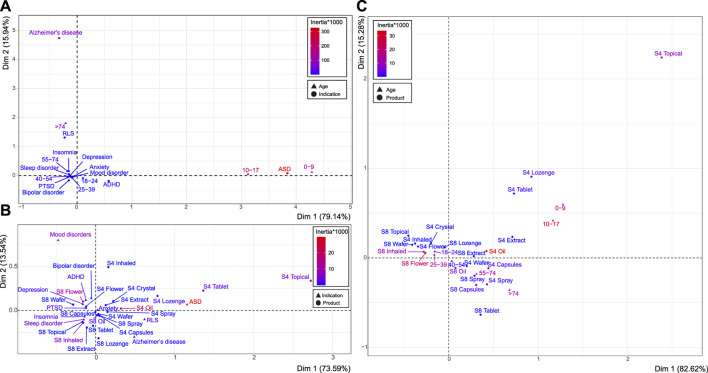
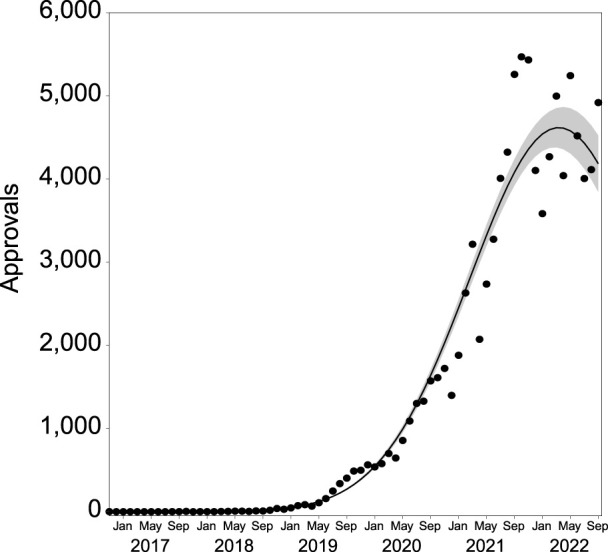
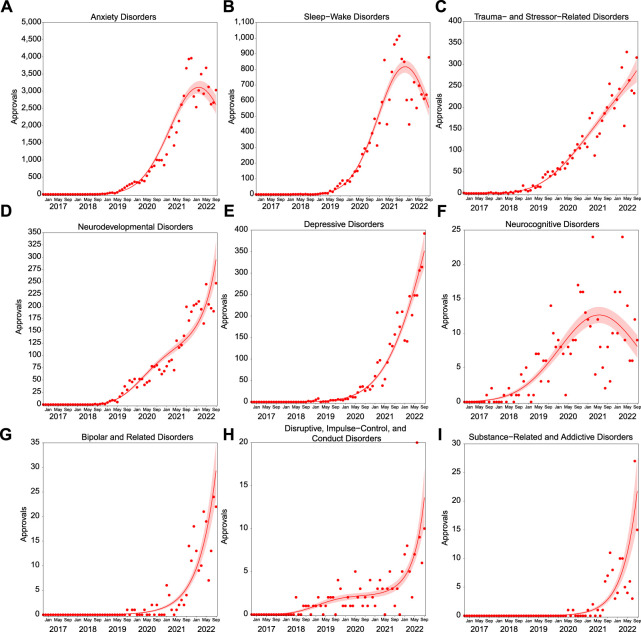
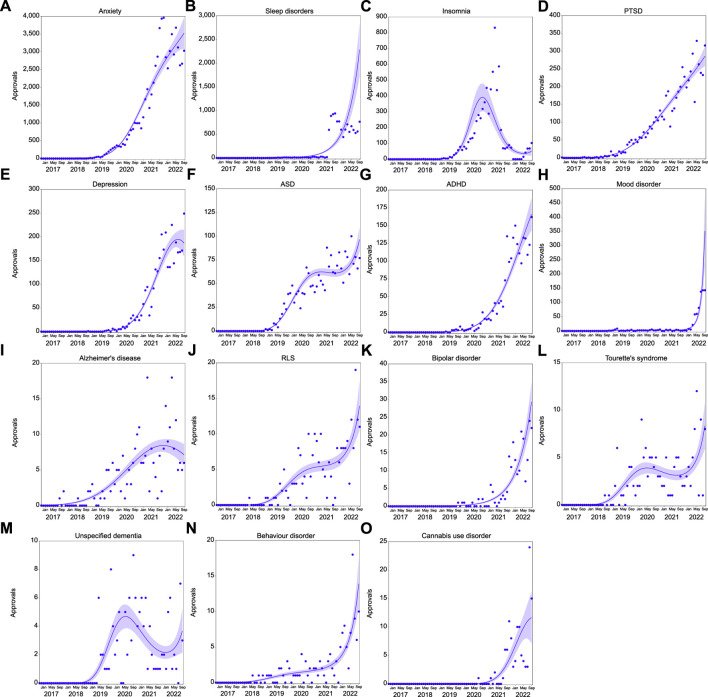
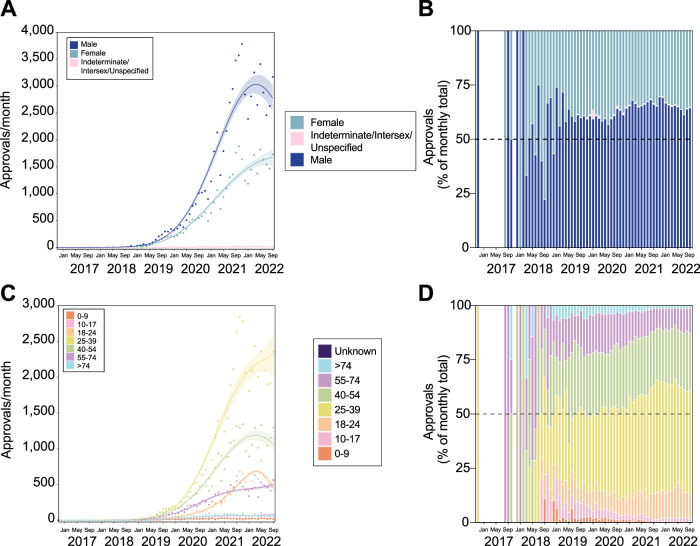
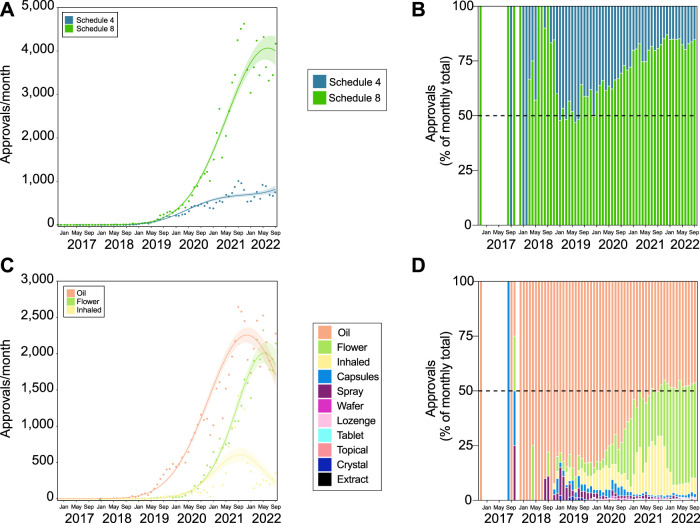
Objective: Evidence is accumulating that components of the Cannabis sativa plant may have therapeutic potential in treating psychiatric disorders. Medicinal cannabis (MC) products are legally available for prescription in Australia, primarily through the Therapeutic Goods Administration (TGA) Special Access Scheme B (SAS-B). Here we investigated recent prescribing practices for psychiatric indications under SAS-B by Australian doctors. Methods: The dataset, obtained from the TGA, included information on MC applications made by doctors through the SAS-B process between 1st November 2016 and 30th September 2022 inclusive. Details included the primary conditions treated, patient demographics, prescriber location, product type (e.g., oil, flower or capsule) and the general cannabinoid content of products. The conditions treated were categorized according to the Diagnostic and Statistical Manual of Mental Disorders, 5th edition, text revision (DSM-5-TR). Trends in prescribing for conditions over time were analyzed via polynomial regression, and relationships between categorical variables determined via correspondence analyses. Results: Approximately 300,000 SAS-B approvals to prescribe MC had been issued in the time period under investigation. This included approvals for 38 different DSM-5-TR defined psychiatric conditions (33.9% of total approvals). The majority of approvals were for anxiety disorders (66.7% of psychiatry-related prescribing), sleep-wake disorders (18.2%), trauma- and stressor-related disorders (5.8%), and neurodevelopmental disorders (4.4%). Oil products were most prescribed (53.0%), followed by flower (31.2%) and other inhaled products (12.4%). CBD-dominant products comprised around 20% of total prescribing and were particularly prevalent in the treatment of autism spectrum disorder. The largest proportion of approvals was for patients aged 25-39 years (46.2% of approvals). Recent dramatic increases in prescribing for attention deficit hyperactivity disorder were identified. Conclusion: A significant proportion of MC prescribing in Australia is for psychiatry-related indications. This prescribing often appears somewhat "experimental", given it involves conditions (e.g., ADHD, depression) for which definitive clinical evidence of MC efficacy is lacking. The high prevalence of THC-containing products being prescribed is of possible concern given the psychiatric problems associated with this drug. Evidence-based clinical guidance around the use of MC products in psychiatry is lacking and would clearly be of benefit to prescribers.
Keywords: Australia; anxiety disorders; medicinal cannabis; medicinal cannabis use; prescribing; psychiatry.
Copyright © 2023 Cairns, Benson, Bedoya-Pérez, Macphail, Mohan, Cohen, Sachdev and McGregor.
Conflict of interest statement
RC reports personal fees from Cannabis Consulting Australia Pty Ltd., personal fees from Biologics Research Institute Australia Pty Ltd., personal fees from University of Sydney, outside the submitted work; IM reports grants from National Health and Medical Research Council of Australia, grants from National Institute of Health, grants from Wellcome Trust, grants and other from University of Sydney (Lambert Initiative), during the course of the study; personal fees from Janssen, outside the submitted work. In addition, IM has patents WO2018107216A1 WO2017004674A1 licensed to Kinoxis Therapeutics, a patent WO2011038451A1 issued, a patent WO2019071302 issued, a patent WO2019227167 issued, a patent AU2017904438 pending, and a patent AU2019051284 pending. PS is supported by an Investigator Grant from the NHMRC, and was on an expert advisory panel for Biogen Australia and Roche Australia in 2020 and 2021. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Appiah-Kusi E., Petros N., Wilson R., Colizzi M., Bossong M. G., Valmaggia L., et al. (2020). Effects of short-term cannabidiol treatment on response to social stress in subjects at clinical high risk of developing psychosis. Psychopharmacol. Berl. 237, 1121–1130. 10.1007/s00213-019-05442-6 - DOI - PMC - PubMed
-
- Arkell T. R., Lintzeris N., Kevin R. C., Ramaekers J. G., Vandrey R., Irwin C., et al. (2019). Cannabidiol (CBD) content in vaporized cannabis does not prevent tetrahydrocannabinol (THC)-induced impairment of driving and cognition. Psychopharmacol. Berl. 236 (9), 2713–2724. 10.1007/s00213-019-05246-8 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources