

Laparoscopic pancreaticoduodenectomy and laparoscopic pancreaticoduodenectomy with robotic reconstruction: single-surgeon experience and technical notes
- PMID: 37347100
- PMCID: PMC10280110
- DOI: 10.7602/jmis.2023.26.2.72
Laparoscopic pancreaticoduodenectomy and laparoscopic pancreaticoduodenectomy with robotic reconstruction: single-surgeon experience and technical notes
Abstract
Purpose: Despite the increasing number of robotic pancreaticoduodenectomies, laparoscopic pancreaticoduodenectomy (LPD) and LPD with robotic reconstruction (LPD-RR) are still valuable surgical options for minimally invasive pancreaticoduodenectomy (MIPD). This study introduces the surgical techniques, tips, and outcomes of our experience with LPD and LPD-RR.
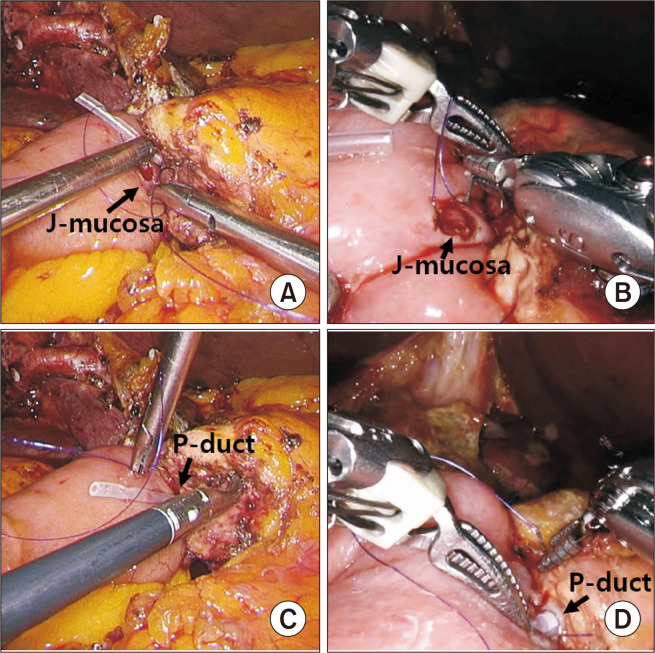
Methods: Between March 2014 and July 2021, 122 and 48 patients underwent LPD and LPD-RR respectively, at CHA Bundang Medical Center in Korea. The operative settings, procedures, and trocar placements were identical in both approaches; however, different trocars were used. We introduced our techniques of retraction methods for Kocherization and uncinate process dissection, pancreatic reconstruction, pancreatic division, and protection using the round ligament. The perioperative surgical outcomes of LPD and LPD-RR were compared.
Results: Baseline demographics of patients in the LPD and LPD-RR groups were comparable, but the LPD group had older age (65.5 ± 11.6 years vs. 60.0 ± 14.1 years, p = 0.009) and lesser preoperative chemotherapy (15.6% vs. 35.4%, p = 0.008). The proportion of malignant disease was similar (LPD group, 86.1% vs. LPD-RR group, 83.3%; p = 0.759). Perioperative outcomes were also comparable, including operative time, estimated blood loss, clinically relevant postoperative pancreatic fistula (LPD group, 9.0% vs. LPD-RR group, 10.4%; p = 0.684), and major postoperative complication rates (LPD group, 14.8% vs. LPD-RR group, 6.2%; p = 0.082).
Conclusion: Both LPD and LPR-RR can be safely performed by experienced surgeons with acceptable surgical outcomes. Further investigations are required to evaluate the objective benefits of robotic surgical systems in MIPD and establish widely acceptable standardized MIPD techniques.
Keywords: Laparoscopy; Minimally invasive surgical procedures; Pancreaticoduodenectomy; Robotics.
© 2023 The Korean Society of Endo-Laparoscopic & Robotic Surgery.
Conflict of interest statement
Conflicts of interest All authors have no conflicts of interest to declare.
Figures




References
-
- van Hilst J, de Rooij T, Bosscha K, et al. Laparoscopic versus open pancreatoduodenectomy for pancreatic or periampullary tumours (LEOPARD-2): a multicentre, patient-blinded, randomised controlled phase 2/3 trial. Lancet Gastroenterol Hepatol. 2019;4:199–207. doi: 10.1016/S2468-1253(19)30004-4. - DOI - PubMed
LinkOut - more resources
Full Text Sources
