

Zygoma implant under function: biomechanical principles clarified
- PMID: 37347335
- PMCID: PMC10287889
- DOI: 10.1186/s40729-023-00483-1
Zygoma implant under function: biomechanical principles clarified
Abstract
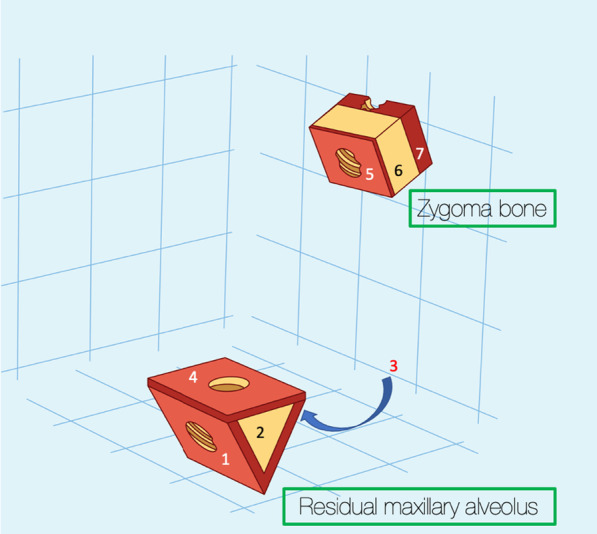
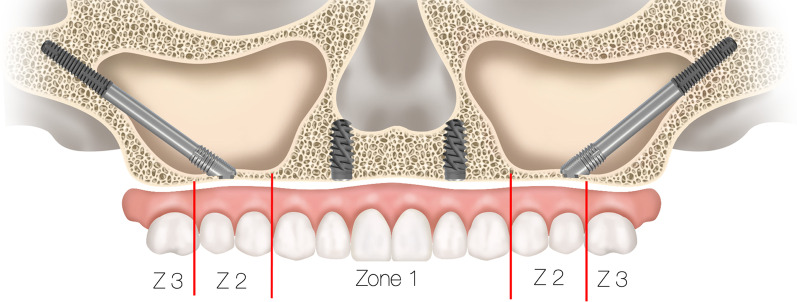
Purpose: The purpose of this document is to clarify the biomechanical principles involved when zygoma implants are placed under functional loads.
Methods: Two independent reviewers conducted electronic search of the literature from January 2000 to February 2023 describing the biomechanical principles involved using the zygoma implant for maxillary reconstruction. Articles describing the stresses within the zygoma implant, the maxillary bone and the zygoma bone under functional loads were included.
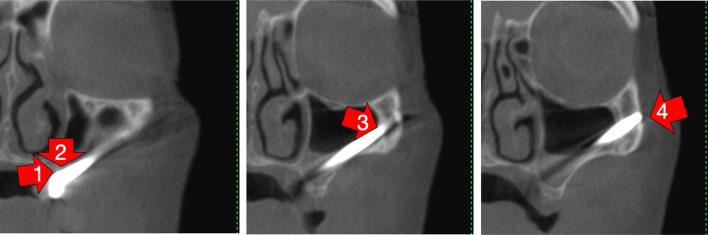
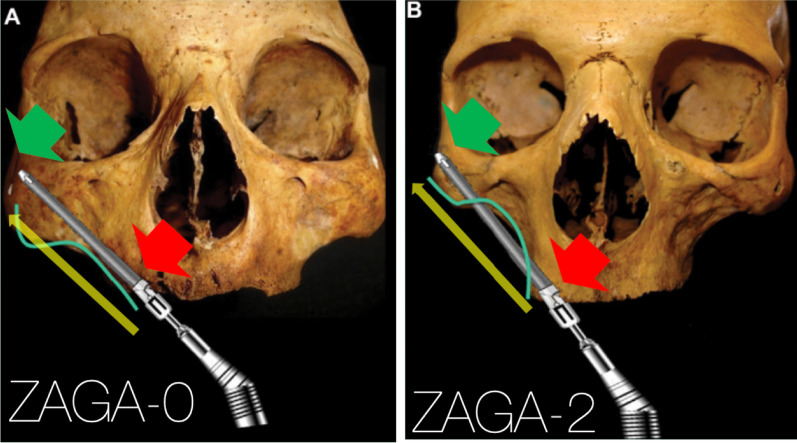
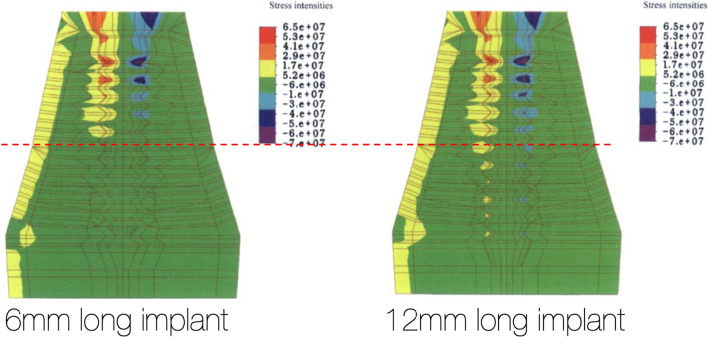
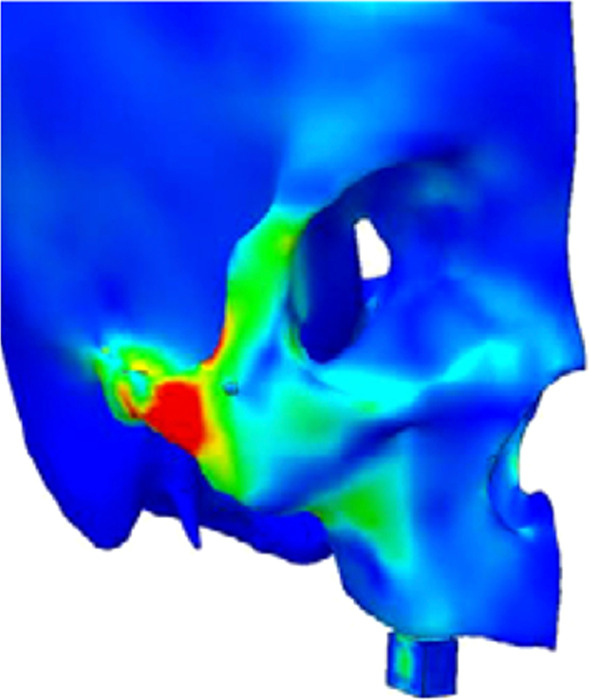
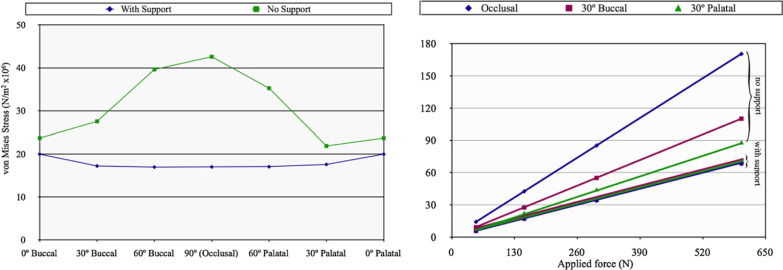
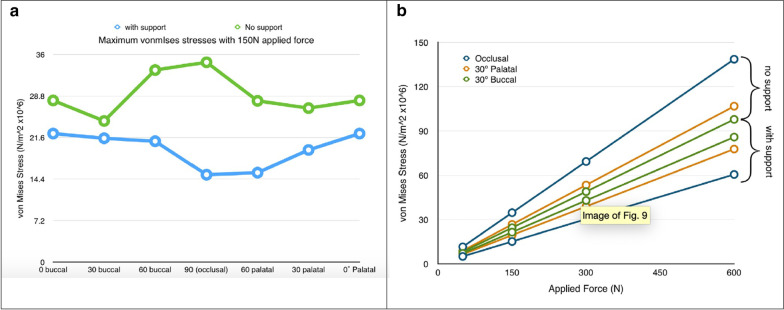
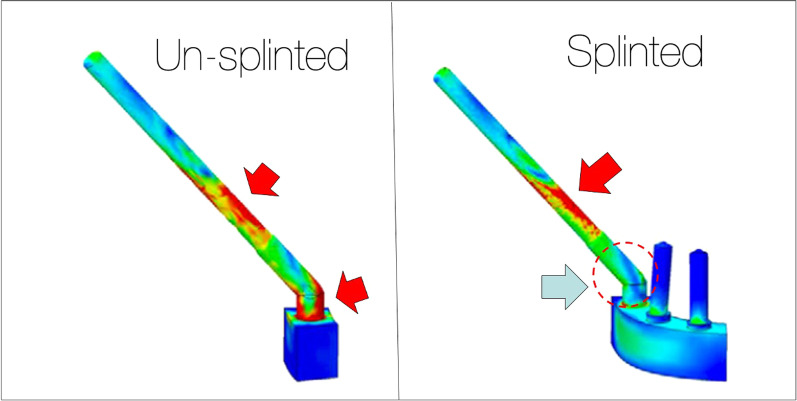
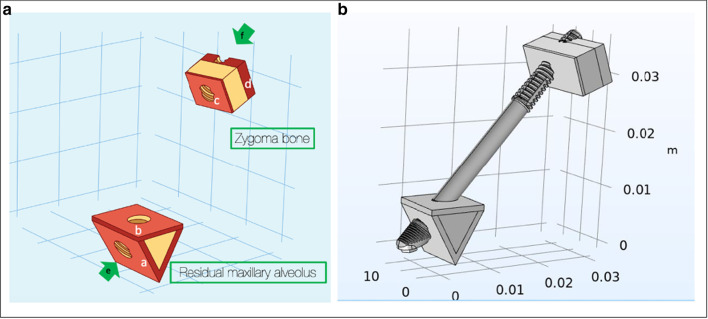
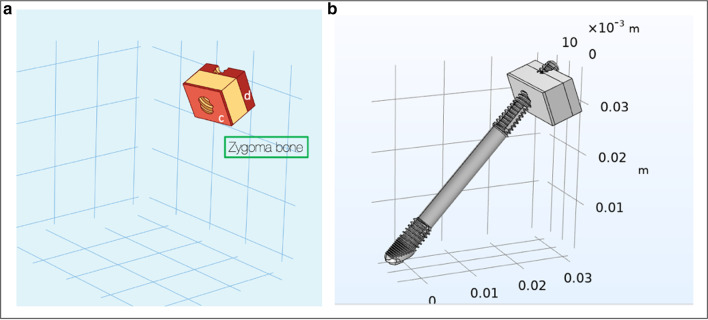
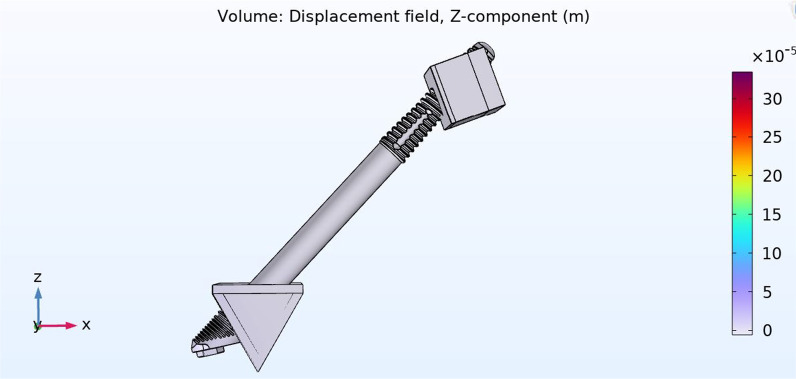
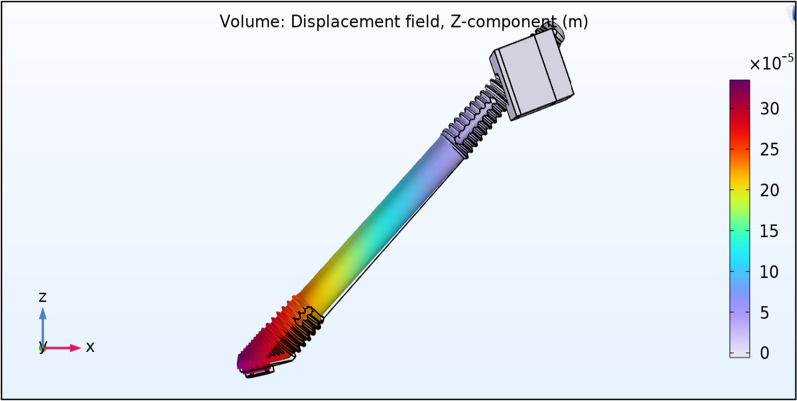
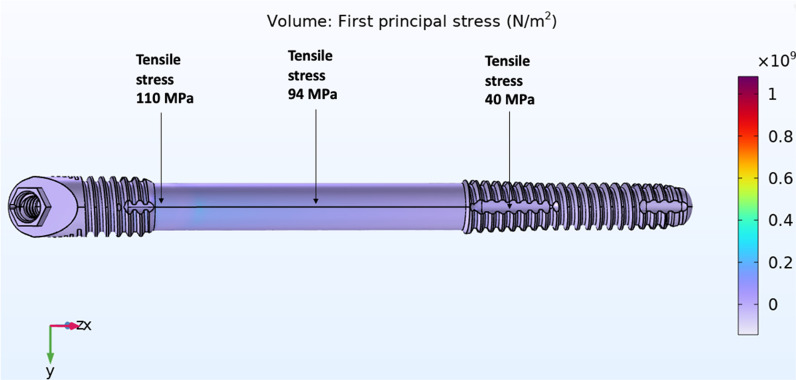
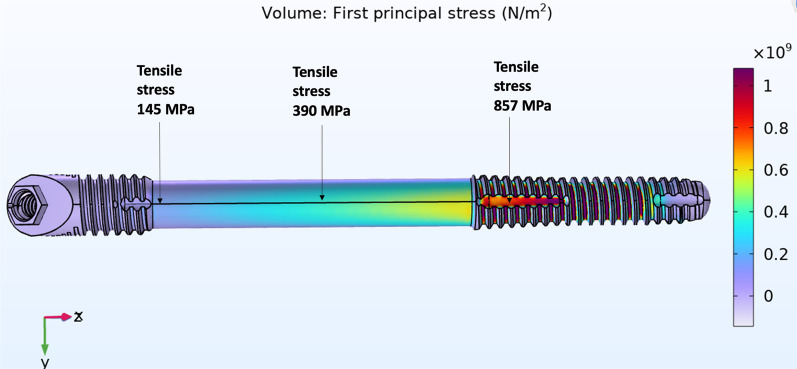
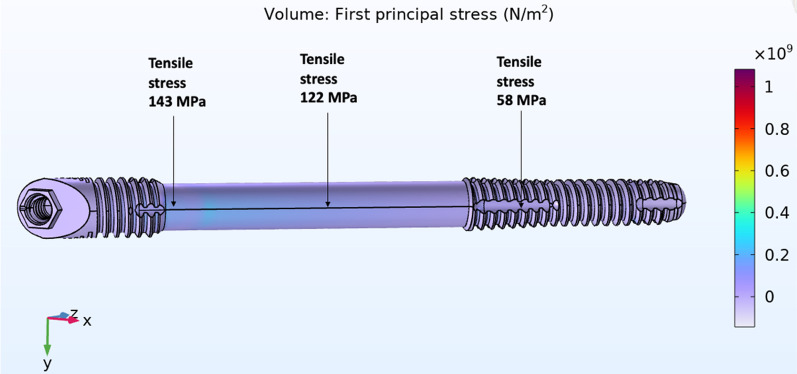
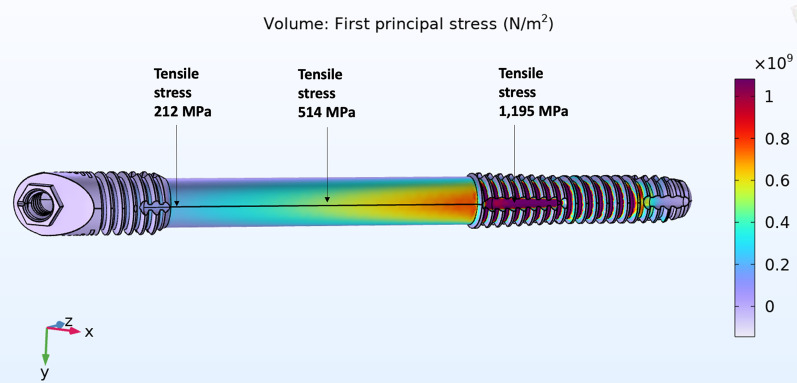
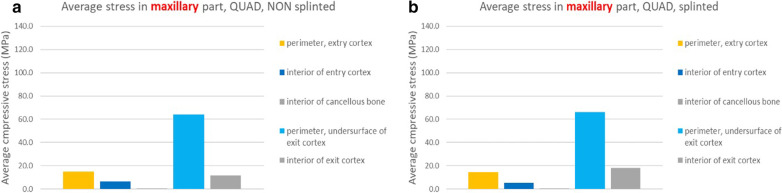
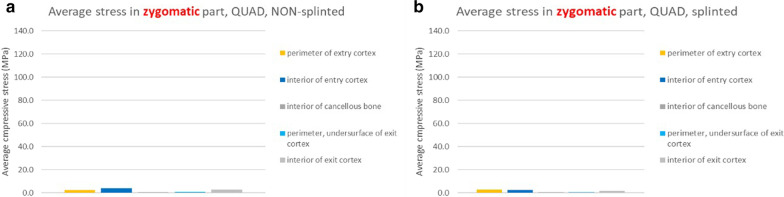
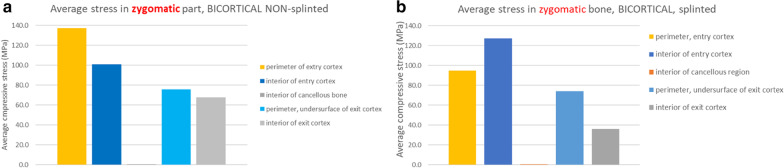
Results: The lack of maxillary boney support at the implant platform resulted in significant higher stress measured within the zygoma implant as well as the zygoma bone.
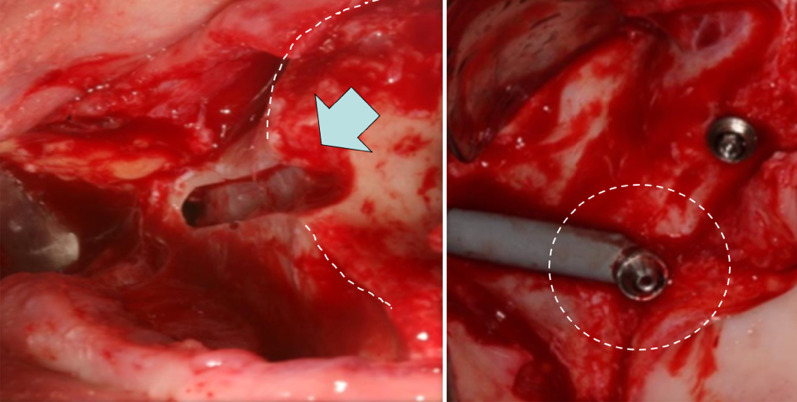
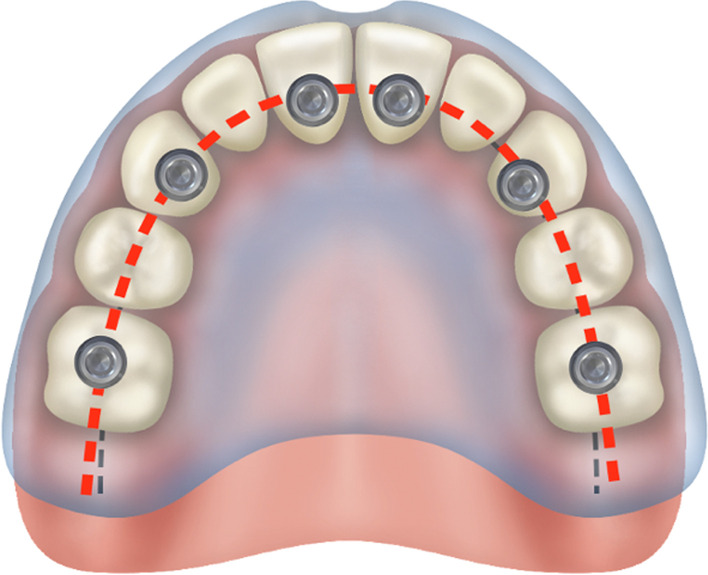
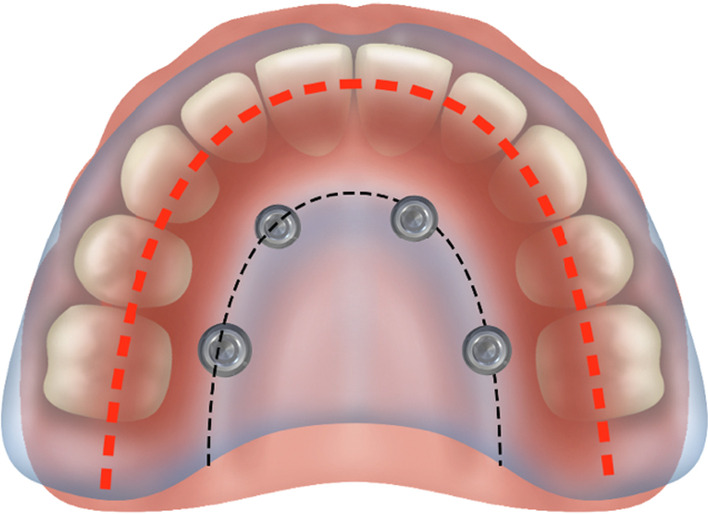
Conclusion: The maxilla is the primary support when zygoma implants are placed under functional loads. Quad-cortical stabilization of the zygoma implants and their cross-arch stabilization are recommended to reduce the degree of stress whenever possible.
© 2023. The Author(s).
Conflict of interest statement
Not applicable.
Figures
References
-
- Brånemark PI, Gröndahl K, Ohrnell LO, Nilsson P, Peterson B, Svensson B, Engstrand P, Nannmark U. Zygoma fixture in the management of advanced atrophy of the maxilla: technique and long-term results. Scand J Plast Reconstr Surg Hand Surg. 2004;38(2):70–85. doi: 10.1080/02844310310023918. - DOI - PubMed
-
- Bedrossian E, Rangers B, Stumpel L, Indersano T. Immediate function with the zygomatic implant: a graftless solution for the patient with mild to advanced atrophy of the maxilla. Int J Oral Maxillofac Implants. 2006;21:937–942. - PubMed
-
- Branemark PI. Surgery and fixture installation: zygomaticus fixture clinical procedures. Gothenburg, Sweden, Nobel Biocare AB; 1998, pp. 1.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
