

Trends in Laboratory-Confirmed SARS-CoV-2 Reinfections and Associated Hospitalizations and Deaths Among Adults Aged ≥18 Years - 18 U.S. Jurisdictions, September 2021-December 2022
- PMID: 37347715
- PMCID: PMC10328471
- DOI: 10.15585/mmwr.mm7225a3
Trends in Laboratory-Confirmed SARS-CoV-2 Reinfections and Associated Hospitalizations and Deaths Among Adults Aged ≥18 Years - 18 U.S. Jurisdictions, September 2021-December 2022
Abstract
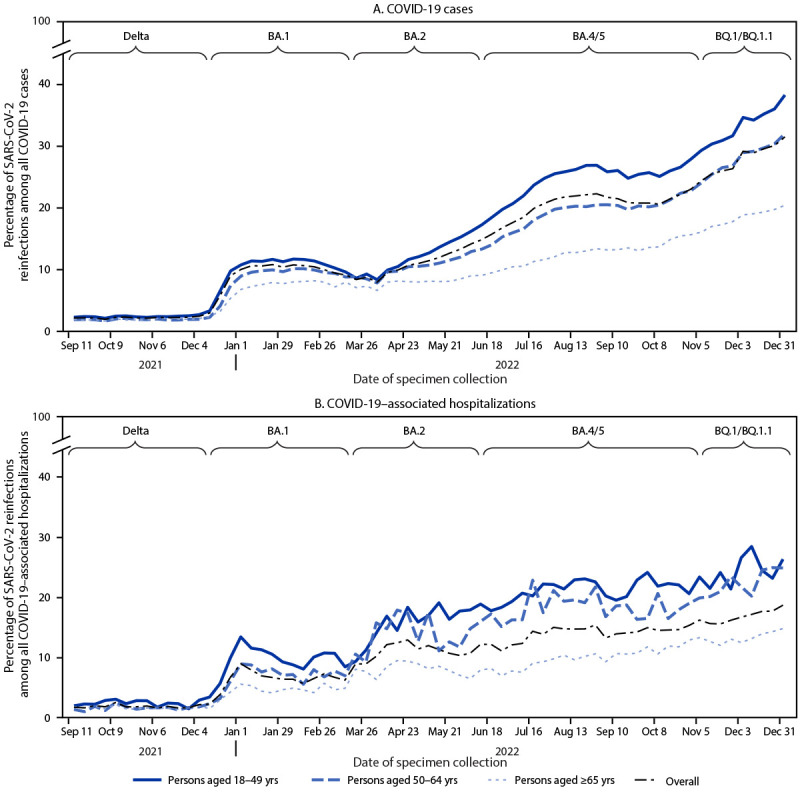
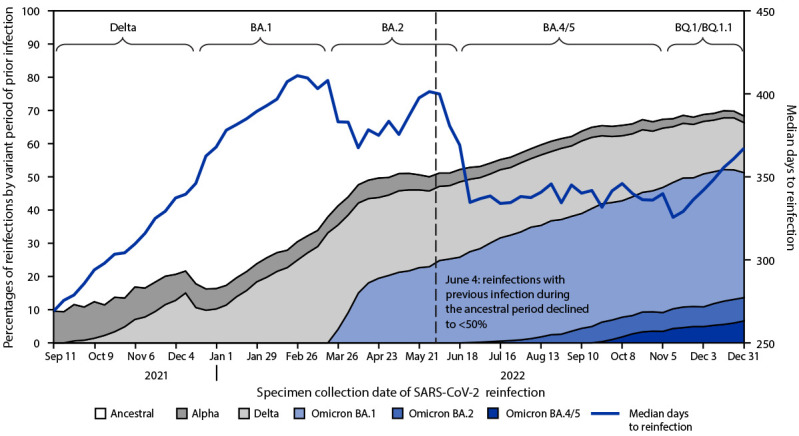
Although reinfections with SARS-CoV-2 have occurred in the United States with increasing frequency, U.S. epidemiologic trends in reinfections and associated severe outcomes have not been characterized. Weekly counts of SARS-CoV-2 reinfections, total infections, and associated hospitalizations and deaths reported by 18 U.S. jurisdictions during September 5, 2021-December 31, 2022, were analyzed overall, by age group, and by five periods of SARS-CoV-2 variant predominance (Delta and Omicron [BA.1, BA.2, BA.4/BA.5, and BQ.1/BQ.1.1]). Among reported reinfections, weekly trends in the median intervals between infections and frequencies of predominant variants during previous infections were calculated. As a percentage of all infections, reinfections increased substantially from the Delta (2.7%) to the Omicron BQ.1/BQ.1.1 (28.8%) periods; during the same periods, increases in the percentages of reinfections among COVID-19-associated hospitalizations (from 1.9% [Delta] to 17.0% [Omicron BQ.1/BQ.1.1]) and deaths (from 1.2% [Delta] to 12.3% [Omicron BQ.1/BQ.1.1]) were also substantial. Percentages of all COVID-19 cases, hospitalizations, and deaths that were reinfections were consistently higher across variant periods among adults aged 18-49 years compared with those among adults aged ≥50 years. The median interval between infections ranged from 269 to 411 days by week, with a steep decline at the start of the BA.4/BA.5 period, when >50% of reinfections occurred among persons previously infected during the Alpha variant period or later. To prevent severe COVID-19 outcomes, including those following reinfection, CDC recommends staying up to date with COVID-19 vaccination and receiving timely antiviral treatments, when eligible.
Conflict of interest statement
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflicts of interest were disclosed.
Figures
References
-
- Hadley E, Yoo YJ, Patel S, et al. SARS-CoV-2 reinfection is preceded by unique biomarkers and related to initial infection timing and severity: an N3C RECOVER EHR-based cohort study. medRxiv [Preprint posted online January 5, 2023]. https://www.medrxiv.org/content/10.1101/2023.01.03.22284042v1 10.1101/2023.01.03.22284042 - DOI
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
