

Interaction of mental comorbidity and physical multimorbidity predicts length-of-stay in medical inpatients
- PMID: 37347745
- PMCID: PMC10287009
- DOI: 10.1371/journal.pone.0287234
Interaction of mental comorbidity and physical multimorbidity predicts length-of-stay in medical inpatients
Abstract
Background: Mental comorbidities of physically ill patients lead to higher morbidity, mortality, health-care utilization and costs.
Objective: The aim of the study was to investigate the impact of mental comorbidity and physical multimorbidity on the length-of-stay in medical inpatients at a maximum-care university hospital.
Design: The study follows a retrospective, quantitative cross-sectional analysis approach to investigate mental comorbidity and physical multimorbidity in internal medicine patients.
Patients: The study comprised a total of n = 28.553 inpatients treated in 2017, 2018 and 2019 at a German Medical University Hospital.
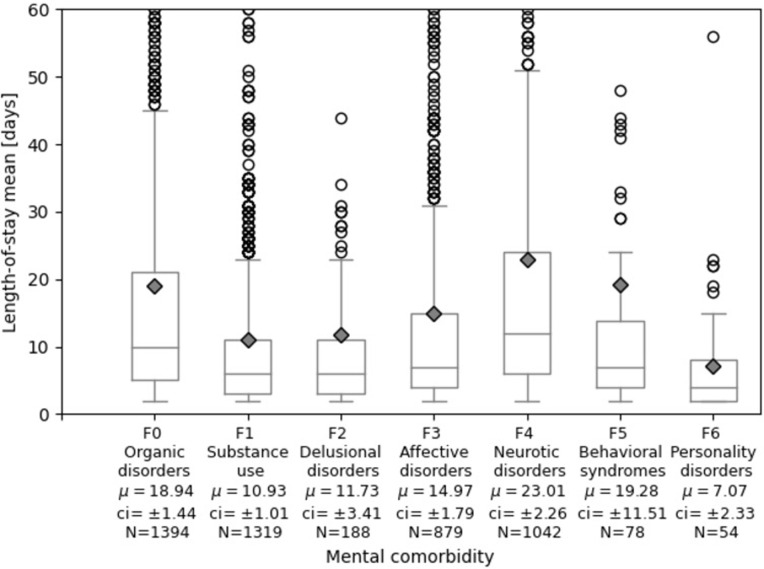
Main measures: Inpatients with a mental comorbidity showed a median length-of-stay of eight days that was two days longer compared to inpatients without a mental comorbidity. Neurotic and somatoform disorders (ICD-10 F4), behavioral syndromes (F5) and organic disorders (F0) were leading with respect to length-of-stay, followed by affective disorders (F3), schizophrenia and delusional disorders (F2), and substance use (F1), all above the sample mean length-of-stay. The impact of mental comorbidity on length-of-stay was greatest for middle-aged patients. Mental comorbidity and Elixhauser score as a measure for physical multimorbidity showed a significant interaction effect indicating that the impact of mental comorbidity on length-of-stay was greater in patients with higher Elixhauser scores.
Conclusions: The findings provide new insights in medical inpatients how mental comorbidity and physical multimorbidity interact with respect to length-of-stay. Mental comorbidity had a large effect on length-of-stay, especially in patients with high levels of physical multimorbidity. Thus, there is an urgent need for new service models to especially care for multimorbid inpatients with mental comorbidity.
Copyright: © 2023 Stahl-Toyota et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



References
-
- Köhle K, Herzog W, Joraschky P, Kruse J, Langewitz W, Söllner W. Uexküll, Psychosomatische Medizin: Theoretische Modelle und klinische Praxis (Engl: Psychosomatic medicine: theoretical models and clinical practice). 8th ed. München: Elsevier; 2017.
-
- Häuser W, Wilhelm-Schwenk R, Klein W, Zimmer C, Krause-Wichmann D. Einfluss psychischer Komorbidität auf die stationäre Verweildauer internistischer Patienten im G-DRG-System (Engl.: Influence of mental comorbidity on the stationary length-of-stay for internistic patients in the G-DRG-System). Psychotherapie, Psychosomatik, medizinische Psychologie. 2006;56(9–10):370–5. doi: 10.1055/s-2006-940179 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
