

Paenibacillus spp infection among infants with postinfectious hydrocephalus in Uganda: an observational case-control study
- PMID: 37348522
- PMCID: PMC10529524
- DOI: 10.1016/S2666-5247(23)00106-4
Paenibacillus spp infection among infants with postinfectious hydrocephalus in Uganda: an observational case-control study
Erratum in
-
Correction to Lancet Microbe 2023; published online June 19. https://doi.org/10.1016/S2666-5247(23)00106-4.Lancet Microbe. 2023 Aug;4(8):e576. doi: 10.1016/S2666-5247(23)00212-4. Epub 2023 Jul 3. Lancet Microbe. 2023. PMID: 37414068 Free PMC article. No abstract available.
Abstract
Background: Paenibacillus thiaminolyticus is a cause of postinfectious hydrocephalus among Ugandan infants. To determine whether Paenibacillus spp is a pathogen in neonatal sepsis, meningitis, and postinfectious hydrocephalus, we aimed to complete three separate studies of Ugandan infants. The first study was on peripartum prevalence of Paenibacillus in mother-newborn pairs. The second study assessed Paenibacillus in blood and cerebrospinal fluid (CSF) from neonates with sepsis. The third study assessed Paenibacillus in CSF from infants with hydrocephalus.
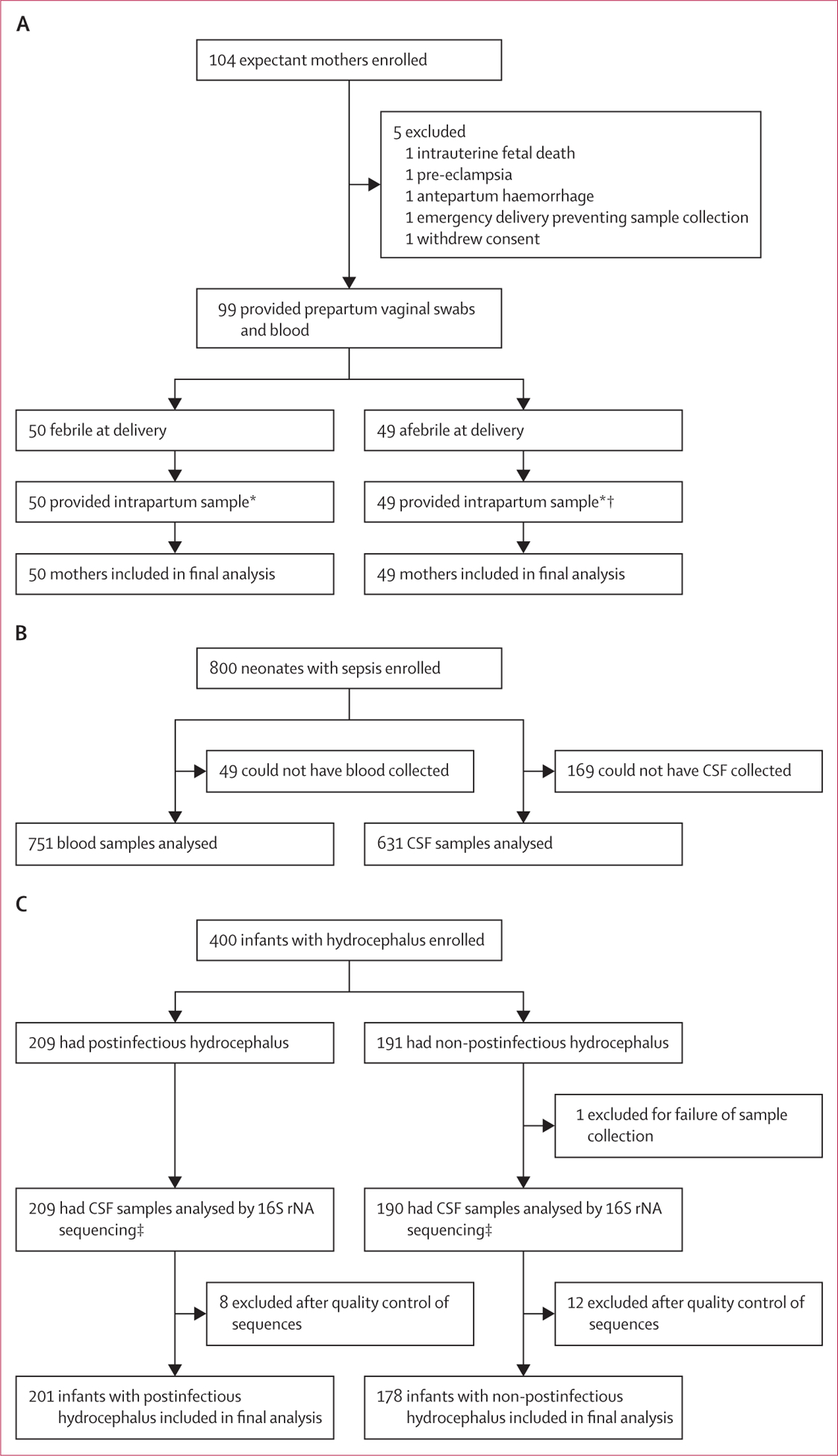
Methods: In this observational study, we recruited mother-newborn pairs with and without maternal fever (mother-newborn cohort), neonates (aged ≤28 days) with sepsis (sepsis cohort), and infants (aged ≤90 days) with hydrocephalus with and without a history of neonatal sepsis and meningitis (hydrocephalus cohort) from three hospitals in Uganda between Jan 13, 2016 and Oct 2, 2019. We collected maternal blood, vaginal swabs, and placental samples and the cord from the mother-newborn pairs, and blood and CSF from neonates and infants. Bacterial content of infant CSF was characterised by 16S rDNA sequencing. We analysed all samples using quantitative PCR (qPCR) targeting either the Paenibacillus genus or Paenibacillus thiaminolyticus spp. We collected cranial ultrasound and computed tomography images in the subset of participants represented in more than one cohort.
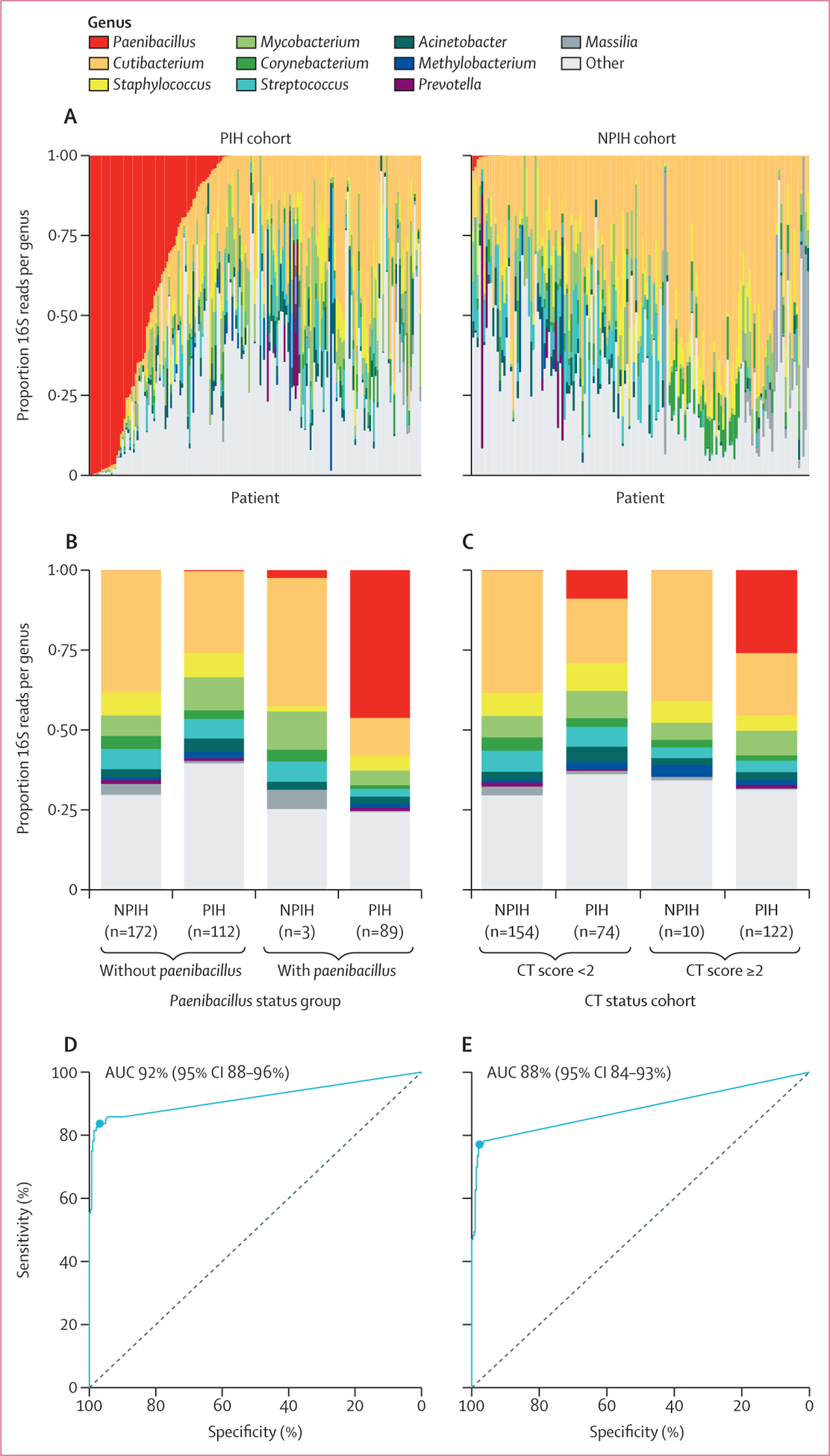
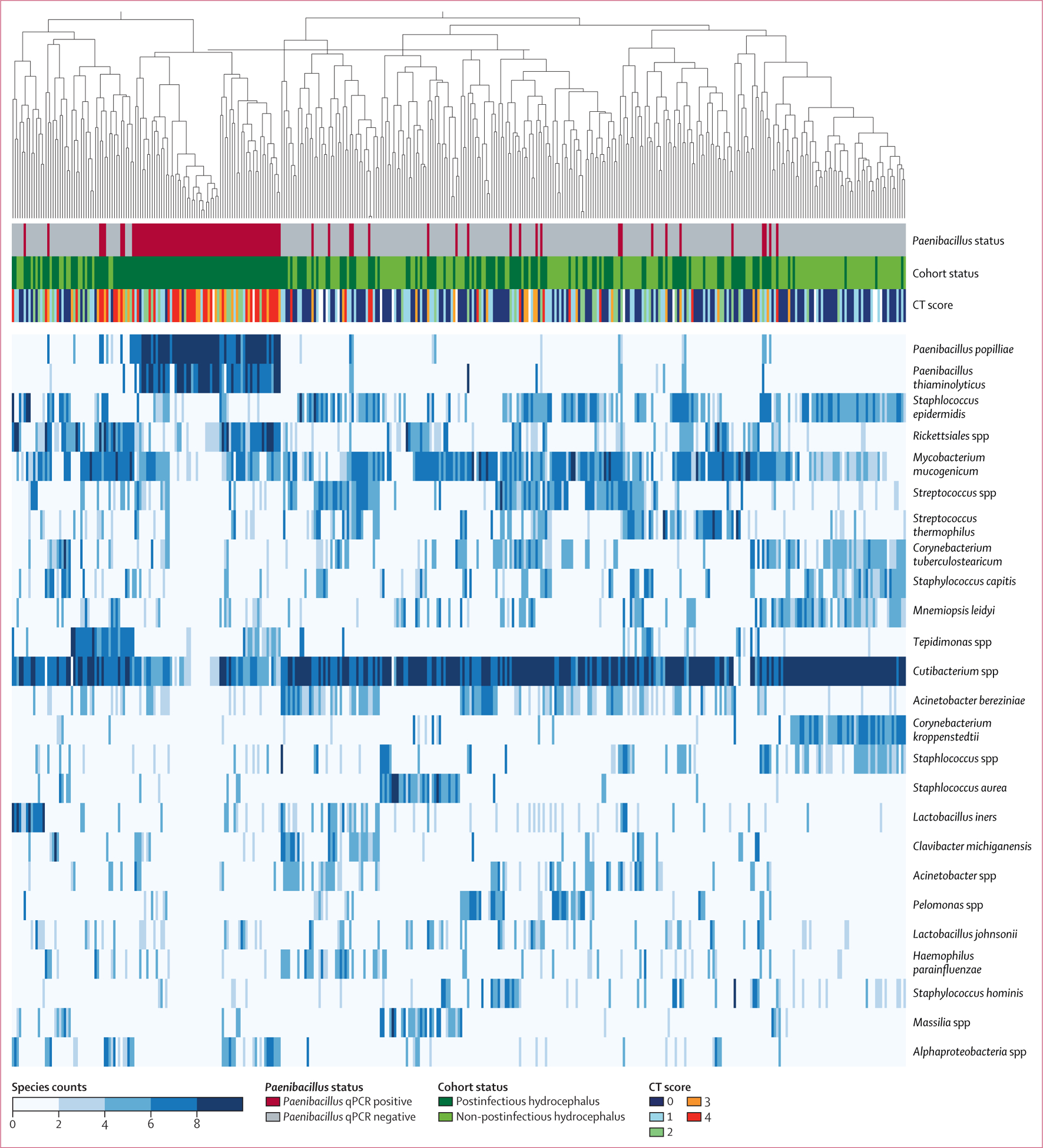
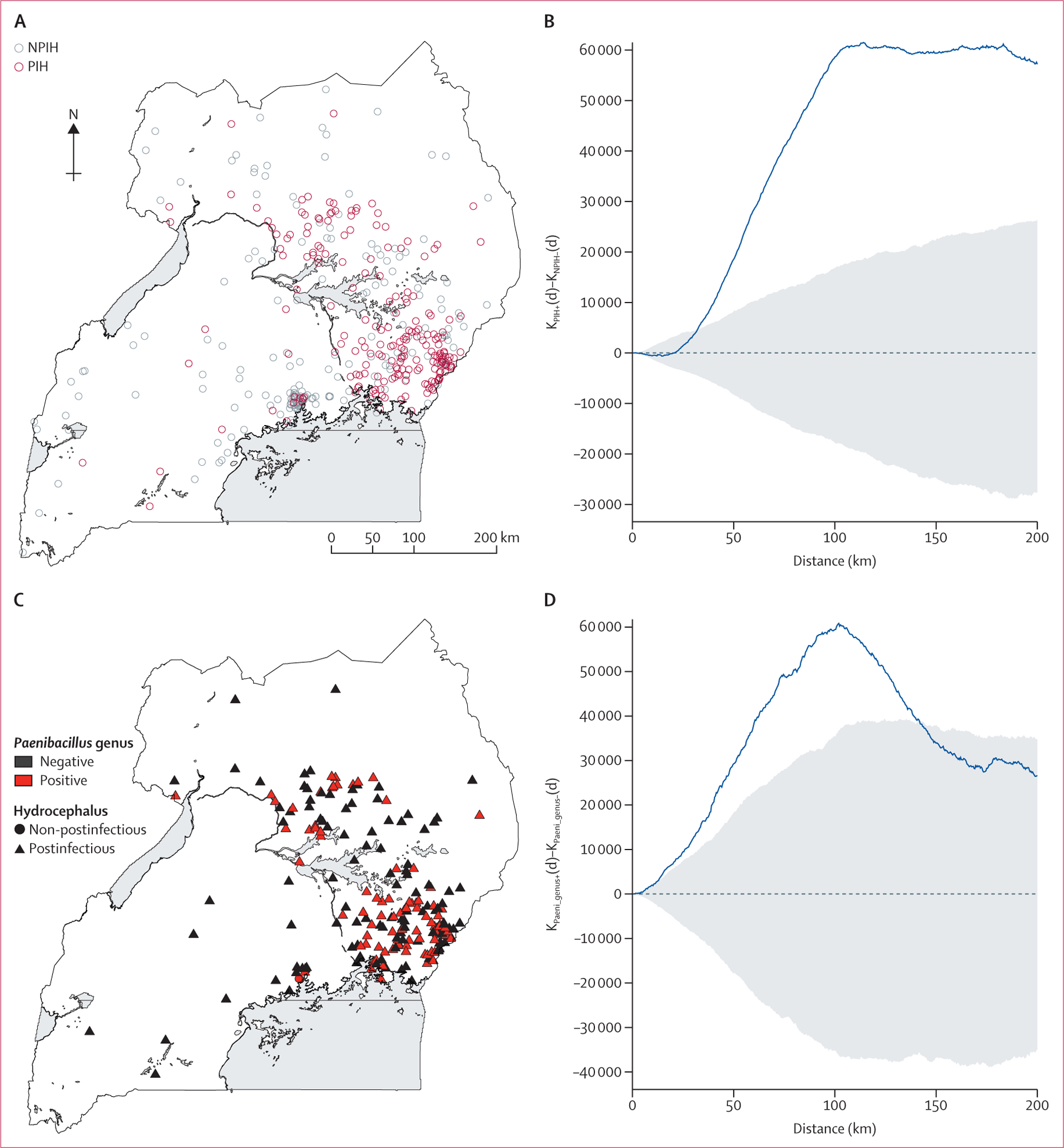
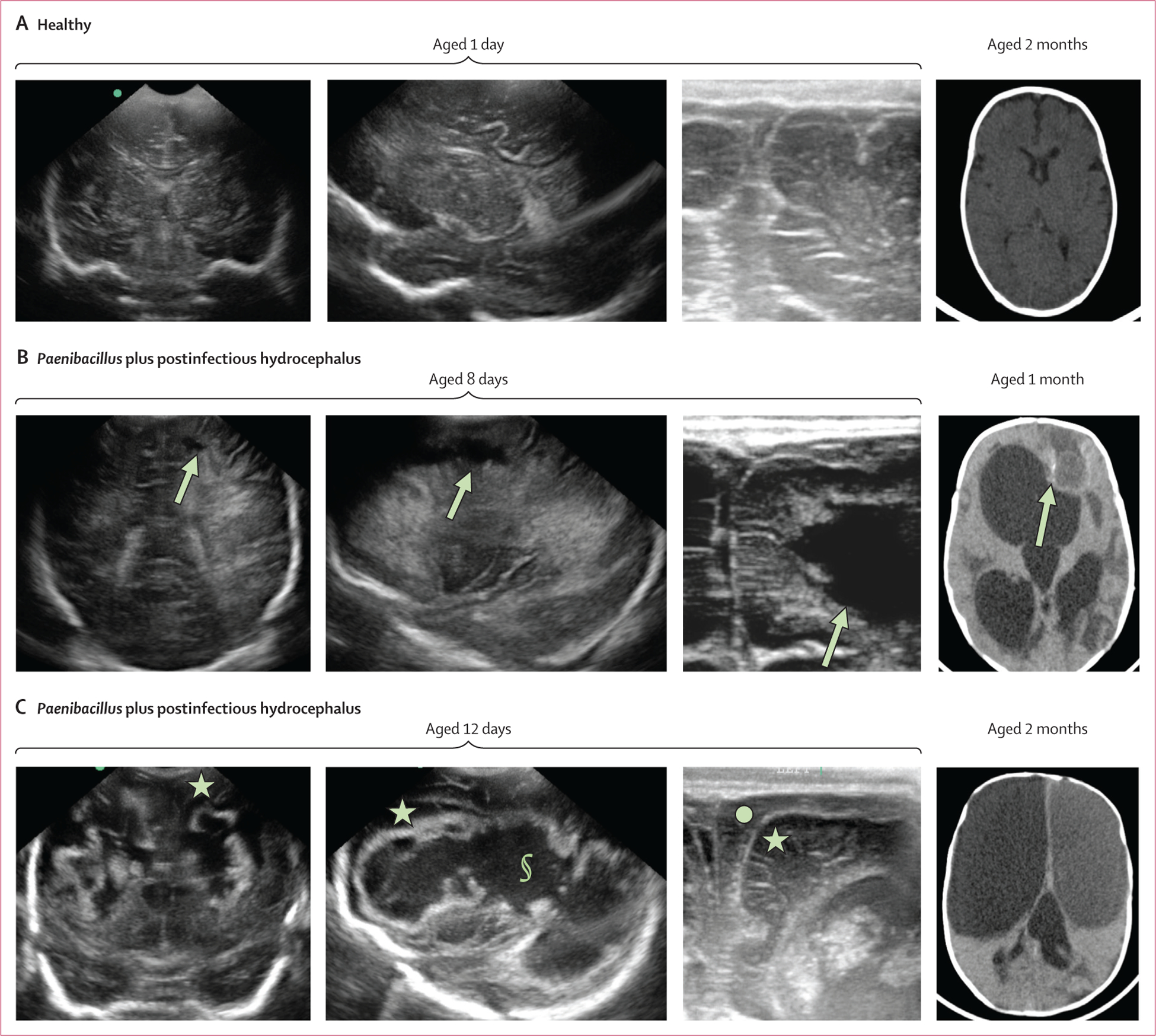
Findings: No Paenibacillus spp were detected in vaginal, maternal blood, placental, or cord blood specimens from the mother-newborn cohort by qPCR. Paenibacillus spp was detected in 6% (37 of 631 neonates) in the sepsis cohort and, of these, 14% (5 of 37 neonates) developed postinfectious hydrocephalus. Paenibacillus was the most enriched bacterial genera in postinfectious hydrocephalus CSF (91 [44%] of 209 patients) from the hydrocephalus cohort, with 16S showing 94% accuracy when validated by qPCR. Imaging showed progression from Paenibacillus spp-related meningitis to postinfectious hydrocephalus over 1-3 months. Patients with postinfectious hydrocephalus with Paenibacillus spp infections were geographically clustered.
Interpretation: Paenibacillus spp causes neonatal sepsis and meningitis in Uganda and is the dominant cause of subsequent postinfectious hydrocephalus. There was no evidence of transplacental transmission, and geographical evidence was consistent with an environmental source of neonatal infection. Further work is needed to identify routes of infection and optimise treatment of neonatal Paenibacillus spp infection to lessen the burden of morbidity and mortality.
Funding: National Institutes of Health and Boston Children's Hospital Office of Faculty Development.
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests KB is Principal Investigator on a Joint Global Health Trials grant from the UK Medical Research Council and has received travel grants and honoraria for speaking at Hot Topics in Neonatology. JEE has received honoraria for participation on the Data Safety Monitoring Board of AbbVie. BCW has received honoraria for participation on the Data Safety Monitoring Board for the Endoscopic versus Shunt Treatment of Hydrocephalus in Infants trial of the Hydrocephalus Clinical Research Network and is the Chairman of Neurokids. JNP has been employed by Genentech and N-Power Medicine; has held stocks and holds and is planning patents at Genentech and N-Power Medicine; has received honoraria for speaking at the International Human Microbiome Consortia meeting; and has received travel support from Genentech. All other authors declare no competing interests. The National Institutes of Health (NIH) Director's Pioneer Award 5DP1HD086071 and NIH Director's Transformative Award 1R01AI145057 has been given to SJS, and the Boston Children's Hospital Office of Faculty Development Career Development Award to SUM. No authors are employed by the NIH.
Figures
Similar articles
-
Neonatal Paenibacilliosis: Paenibacillus Infection as a Novel Cause of Sepsis in Term Neonates With High Risk of Sequelae in Uganda.Clin Infect Dis. 2023 Sep 11;77(5):768-775. doi: 10.1093/cid/ciad337. Clin Infect Dis. 2023. PMID: 37279589 Free PMC article.
-
Cytomegalovirus infections in infants in Uganda: Newborn-mother pairs, neonates with sepsis, and infants with hydrocephalus.Int J Infect Dis. 2022 May;118:24-33. doi: 10.1016/j.ijid.2022.02.005. Epub 2022 Feb 9. Int J Infect Dis. 2022. PMID: 35150915 Free PMC article.
-
Paenibacillus infection with frequent viral coinfection contributes to postinfectious hydrocephalus in Ugandan infants.Sci Transl Med. 2020 Sep 30;12(563):eaba0565. doi: 10.1126/scitranslmed.aba0565. Sci Transl Med. 2020. PMID: 32998967 Free PMC article.
-
Proposal of "evolution theory in cerebrospinal fluid dynamics" and minor pathway hydrocephalus in developing immature brain.Childs Nerv Syst. 2006 Jul;22(7):662-9. doi: 10.1007/s00381-005-0020-4. Epub 2006 May 10. Childs Nerv Syst. 2006. PMID: 16685545 Review.
-
Long-term impact of serious neonatal bacterial infections on neurodevelopment.Clin Microbiol Infect. 2024 Jan;30(1):28-37. doi: 10.1016/j.cmi.2023.04.017. Epub 2023 Apr 19. Clin Microbiol Infect. 2024. PMID: 37084940 Review.
Cited by
-
The choroid plexus synergizes with immune cells during neuroinflammation.Cell. 2024 Sep 5;187(18):4946-4963.e17. doi: 10.1016/j.cell.2024.07.002. Epub 2024 Jul 31. Cell. 2024. PMID: 39089253
-
Paediatric hydrocephalus.Nat Rev Dis Primers. 2024 May 16;10(1):35. doi: 10.1038/s41572-024-00519-9. Nat Rev Dis Primers. 2024. PMID: 38755194 Free PMC article. Review.
-
A Systematic Review of Human Paenibacillus Infections and Comparison of Adult and Pediatric Cases.Pediatr Infect Dis J. 2025 May 1;44(5):455-461. doi: 10.1097/INF.0000000000004668. Epub 2024 Dec 18. Pediatr Infect Dis J. 2025. PMID: 39705610
-
Poor surgical outcomes following Paenibacillus infant infectious hydrocephalus.J Neurosurg Pediatr. 2025 May 16;36(2):145-156. doi: 10.3171/2025.1.PEDS24254. Print 2025 Aug 1. J Neurosurg Pediatr. 2025. PMID: 40378477
-
Five-year outcomes after surgical treatment of infant postinfectious hydrocephalus in sub-Saharan Africa: results of a randomized trial.J Neurosurg Pediatr. 2025 May 2;36(2):135-144. doi: 10.3171/2025.1.PEDS24417. Print 2025 Aug 1. J Neurosurg Pediatr. 2025. PMID: 40315611 Clinical Trial.
References
-
- Alkema L, Chao F, You D, Pedersen J, Sawyer CC. National, regional, and global sex ratios of infant, child, and under-5 mortality and identification of countries with outlying ratios: a systematic assessment. Lancet Glob Health 2014; 2: e521–30. - PubMed
-
- Dewan MC, Rattani A, Mekary R, et al. Global hydrocephalus epidemiology and incidence: systematic review and meta-analysis. J Neurosurg 2018; 130: 1–15. - PubMed
-
- Warf BC. Hydrocephalus in Uganda: the predominance of infectious origin and primary management with endoscopic third ventriculostomy. J Neurosurg 2005; 102: 1–15. - PubMed
-
- Warf BC, Dagi AR, Kaaya BN, Schiff SJ. Five-year survival and outcome of treatment for postinfectious hydrocephalus in Ugandan infants. J Neurosurg Pediatr 2011; 8: 502–08. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
