

Intravenous aviptadil and remdesivir for treatment of COVID-19-associated hypoxaemic respiratory failure in the USA (TESICO): a randomised, placebo-controlled trial
- PMID: 37348524
- PMCID: PMC10527239
- DOI: 10.1016/S2213-2600(23)00147-9
Intravenous aviptadil and remdesivir for treatment of COVID-19-associated hypoxaemic respiratory failure in the USA (TESICO): a randomised, placebo-controlled trial
Abstract
Background: There is a clinical need for therapeutics for COVID-19 patients with acute hypoxemic respiratory failure whose 60-day mortality remains at 30-50%. Aviptadil, a lung-protective neuropeptide, and remdesivir, a nucleotide prodrug of an adenosine analog, were compared with placebo among patients with COVID-19 acute hypoxaemic respiratory failure.
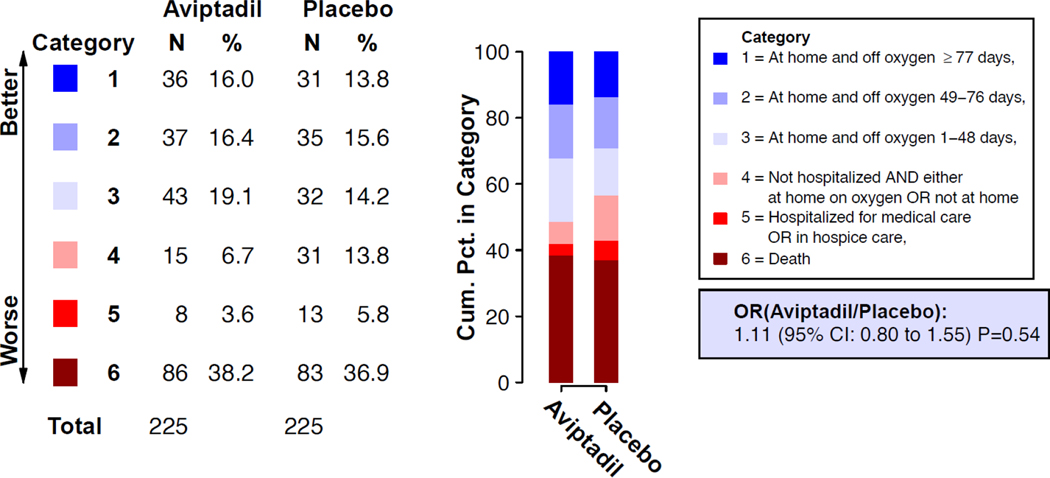
Methods: TESICO was a randomised trial of aviptadil and remdesivir versus placebo at 28 sites in the USA. Hospitalised adult patients were eligible for the study if they had acute hypoxaemic respiratory failure due to confirmed SARS-CoV-2 infection and were within 4 days of the onset of respiratory failure. Participants could be randomly assigned to both study treatments in a 2 × 2 factorial design or to just one of the agents. Participants were randomly assigned with a web-based application. For each site, randomisation was stratified by disease severity (high-flow nasal oxygen or non-invasive ventilation vs invasive mechanical ventilation or extracorporeal membrane oxygenation [ECMO]), and four strata were defined by remdesivir and aviptadil eligibility, as follows: (1) eligible for randomisation to aviptadil and remdesivir in the 2 × 2 factorial design; participants were equally randomly assigned (1:1:1:1) to intravenous aviptadil plus remdesivir, aviptadil plus remdesivir matched placebo, aviptadil matched placebo plus remdesvir, or aviptadil placebo plus remdesivir placebo; (2) eligible for randomisation to aviptadil only because remdesivir was started before randomisation; (3) eligible for randomisation to aviptadil only because remdesivir was contraindicated; and (4) eligible for randomisation to remdesivir only because aviptadil was contraindicated. For participants in strata 2-4, randomisation was 1:1 to the active agent or matched placebo. Aviptadil was administered as a daily 12-h infusion for 3 days, targeting 600 pmol/kg on infusion day 1, 1200 pmol/kg on day 2, and 1800 pmol/kg on day 3. Remdesivir was administered as a 200 mg loading dose, followed by 100 mg daily maintenance doses for up to a 10-day total course. For participants assigned to placebo for either agent, matched saline placebo was administered in identical volumes. For both treatment comparisons, the primary outcome, assessed at day 90, was a six-category ordinal outcome: (1) at home (defined as the type of residence before hospitalisation) and off oxygen (recovered) for at least 77 days, (2) at home and off oxygen for 49-76 days, (3) at home and off oxygen for 1-48 days, (4) not hospitalised but either on supplemental oxygen or not at home, (5) hospitalised or in hospice care, or (6) dead. Mortality up to day 90 was a key secondary outcome. The independent data and safety monitoring board recommended stopping the aviptadil trial on May 25, 2022, for futility. On June 9, 2022, the sponsor stopped the trial of remdesivir due to slow enrolment. The trial is registered with ClinicalTrials.gov, NCT04843761.
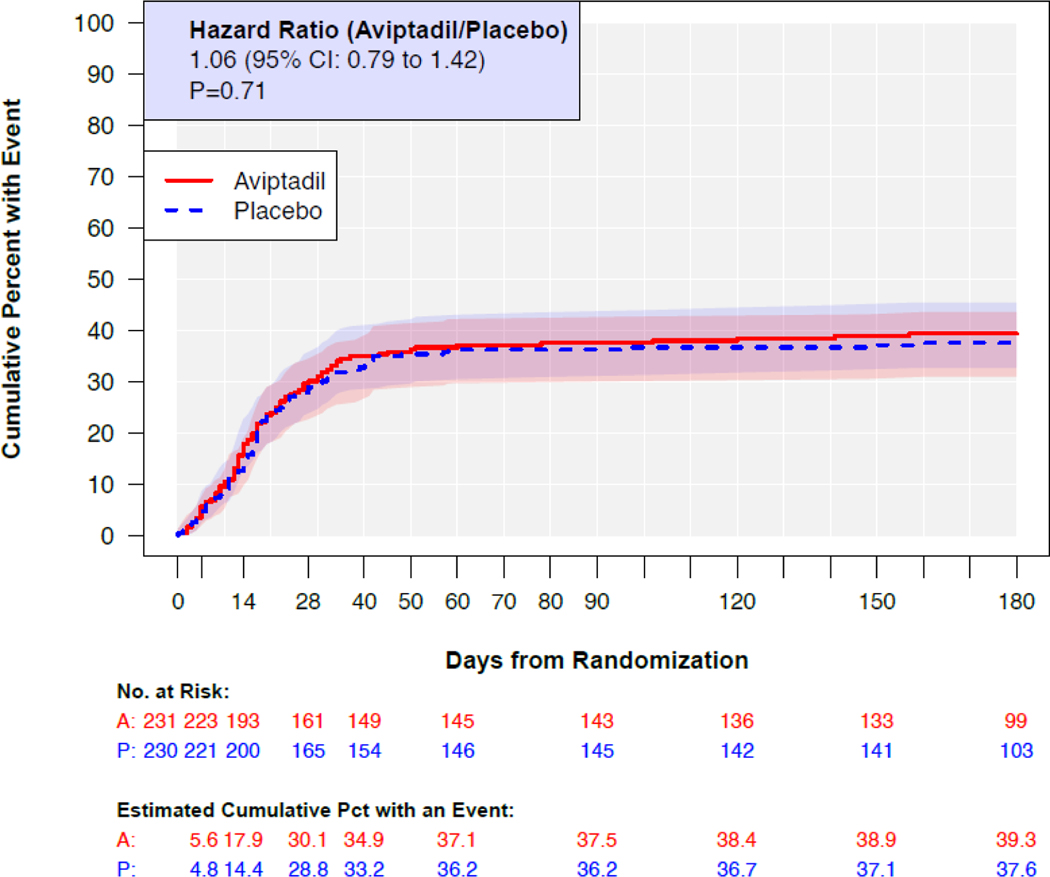
Findings: Between April 21, 2021, and May 24, 2022, we enrolled 473 participants in the study. For the aviptadil comparison, 471 participants were randomly assigned to aviptadil or matched placebo. The modified intention-to-treat population comprised 461 participants who received at least a partial infusion of aviptadil (231 participants) or aviptadil matched placebo (230 participants). For the remdesivir comparison, 87 participants were randomly assigned to remdesivir or matched placebo and all received some infusion of remdesivir (44 participants) or remdesivir matched placebo (43 participants). 85 participants were included in the modified intention-to-treat analyses for both agents (ie, those enrolled in the 2 x 2 factorial). For the aviptadil versus placebo comparison, the median age was 57 years (IQR 46-66), 178 (39%) of 461 participants were female, and 246 (53%) were Black, Hispanic, Asian or other (vs 215 [47%] White participants). 431 (94%) of 461 participants were in an intensive care unit at baseline, with 271 (59%) receiving high-flow nasal oxygen or non-invasive ventiliation, 185 (40%) receiving invasive mechanical ventilation, and five (1%) receiving ECMO. The odds ratio (OR) for being in a better category of the primary efficacy endpoint for aviptadil versus placebo at day 90, from a model stratified by baseline disease severity, was 1·11 (95% CI 0·80-1·55; p=0·54). Up to day 90, 86 participants in the aviptadil group and 83 in the placebo group died. The cumulative percentage who died up to day 90 was 38% in the aviptadil group and 36% in the placebo group (hazard ratio 1·04, 95% CI 0·77-1·41; p=0·78). The primary safety outcome of death, serious adverse events, organ failure, serious infection, or grade 3 or 4 adverse events up to day 5 occurred in 146 (63%) of 231 patients in the aviptadil group compared with 129 (56%) of 230 participants in the placebo group (OR 1·40, 95% CI 0·94-2·08; p=0·10).
Interpretation: Among patients with COVID-19-associated acute hypoxaemic respiratory failure, aviptadil did not significantly improve clinical outcomes up to day 90 when compared with placebo. The smaller than planned sample size for the remdesivir trial did not permit definitive conclusions regarding safety or efficacy.
Funding: National Institutes of Health.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests SMB reports funding from the National Institutes of Health during the conduct of the study and chairing a Data and Safety Monitoring Board (DSMB) for Hamilton Ventilators, outside of the study. CEB reports funding from the National Institutes of Health (NIH) for the Aviptadil study, during the conduct of the study. BG reports grants from the NIH, during the conduct of the study. SS reports a grant from the NIH, during the conduct of the study. ANP reports grants from the Wellcome Trust, the National Institute for Health and Care Research, UK Research and Innovation (UKRI), and the Bill & Melinda Gates Foundation, and consulting fees from the Bill & Melinda Gates Foundation, outside of the submitted work. IDP reports funding from NIH and the National Institute of General Medical Sciences, during the conduct of the study, a grant from Janssen for a study of influenza patient reported outcomes, and a contract with Regeneron for a COVID-19 therapy trial, outside of the submitted work. JRB reports a grant from the NIH, during the conduct of the study, grants from the NIH, Quantum Leap Healthcare Collaborative, and Sedana Medical, consulting fees from Sedana Medical, Biomarck, and Global Blood Therapeutics, and compensation from Hamilton Medical for participation as a medical monitor, outside of the submitted work. ESHa reports study materials from NeuroRx and Gilead through a National Heart, Lung, and Blood Institute (NHLBI) subcontract, during the conduct of the study, subcontracts with Bristol Meyers Squibb (BMS), Allergan, Gilead, and Janssen for the Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV-1) clinical trial, subcontracts with AstraZeneca, Brii Biosciences, Vir Biotechnology, and Eli Lilly for the Therapeutics for Inpatients with COVID-19 (TICO) clinical trial, and additional subcontracts with Rigel, APEIRON Biologics, and Trevena for the Novel Experimental COVID-19 Therapies Affecting Host Response (NECTAR) clinical trial, outside of the submitted work. EAM reports study materials from NeuroRx and Gilead through an NHLBI subcontract, during the conduct of the study, subcontracts with BMS, Allergan, Gilead, and Janssen for the ACTIV-1 clinical trial, subcontracts with AstraZeneca, Brii Biosciences, Vir Biotechnology, and Eli Lilly for the TICO clinical trial, and additional subcontracts with Rigel, APEIRON Biologics, and Trevena for the NECTAR clinical trial, outside of the submitted work. MAGB reports study materials from NeuroRx and Gilead through an NHLBI subcontract, during the conduct of the study, subcontracts with BMS, Allergan, Gilead, and Janssen for the ACTIV-1 clinical trial, subcontracts with AstraZeneca, Brii Biosciences, Vir Biotechnology, and Eli Lilly for the TICO clinical trial, and subcontracts with Rigel, APEIRON Biologics, and Trevena for the NECTAR clinical trial, outside of the submitted work. KSM reports grants and contracts from NIH, NHLBI, and the Society for Critical Care Medicine, participation as a steering committee member for Roivant-Kinevant Sciences, and employment as a clinical research physician at Chiesi USA, outside of submitted work. JM reports receiving study materials and funding from the Albert Einstein College of Medicine for the study protocol, during the conduct of the study. CH reports funding from the National Institute of Allergy and Infectious Diseases (NIAID) in the form of per-patient payments for A Multicenter, Adaptive, Randomized, Blinded Controlled Trial of the Safety and Efficacy of Investigational Therapeutics for Hospitalized Patients with Acute Respiratory Distress Syndrome Associated with COVID-19, during the conduct of the study. AK reports grants from Eli Lilly, AstraZeneca, 4D Medical, United Therapeutics, Regeneron Pharmaceuticals, and Dompe Pharmaceuticals and consulting fees from Dompe Pharmaceuticals for clinical trial design, outside of the submitted work. AD reports grants from NHLBI Prevention and Early Treatment of Acute Lung Injury network and the US Centers for Disease Control and Prevention (CDC) and data safety monitoring board (DSMB) or advisory board participation for Alung Technologies, outside of the submitted work. SD reports a grant from Chest Sonosite Ultrasound to study the incidence of deep vein thrombosis in patients with COVID-19, during the conduct of the study. AJG reports payment from Sound Pharmaceuticals for participation as a medical monitor for a COVID therapeutic trial, outside of the submitted work. USS reports consulting fees from Shionogi, Paratek, and ViiV Healthcare for participation on advisory boards and speaking fees from Shionogi and Paratek, outside of the submitted work. NJJ reports grants from the CDC, the US Department of Defense (DOD), and NIH and participation on a DSMB for the Legacy Health System, outside of the submitted work. MAM reports grants from NIH and NIAID, during the conduct of the study. NRA reports funding from NIH, during the conduct of the study. JDC reports grants from NIH and DOD, outside of the submitted work. DDM reports funding from the Danish National Research Foundation (DNRF126), during the conduct of study. AAG reports funding from NIH, during the conduct of the study, grants or contracts from NIH, DOD, CDC, Faron Pharmaceuticals, and Abbvie, and participation on a DSMB or advisory board for NIH, outside of the submitted work. WHS reports funding from NIH and NIAID, during the conduct of the study. CFO reports contracts with NIH and NHLBI, outside of the submitted work. BTT reports a grant from NHLBI, consulting fees from Bayer, Genetec, and Novartis, and participation on a DSMB or advisory board for Aperion, outside of the submitted work. During a portion of this research, BTT had a financial interest in Direct Biologics, a developer and manufacturer of regenerative biologic products, including an investigational treatment of COVID-19-associated ARDS. BTT's interests were reviewed and are managed by Massachusetts General Hospital and Mass General Brigham in accordance with their conflict of interest policies, and had no relationship to the agents studied. VK reports subcontracts with University of Minnesota, NIAID, and NIH for the TICO and Therapeutics for Severely Ill Inpatients with COVID-19 platform trials, outside of the submitted work. AGB reports a grant from University of Minnesota, during the conduct of the study, grants from the Medical Reserve Corps and UKRI, payment from NIAID for participation on a COVID-19 Vaccines DSMB, and participation on the WHO Trial Data and Safety Monitoring Committee, outside of the submitted work. JDN reports grants from NIAID, NIH, and Leidos Biomedical, outside of the submitted work. HCL reports employment from NIAID, during the conduct of the study. All other authors declare no competing interests.
Figures
Comment in
-
A negative trial for vasoactive intestinal peptide in COVID-19-associated acute hypoxaemic respiratory failure.Lancet Respir Med. 2023 Sep;11(9):759-760. doi: 10.1016/S2213-2600(23)00218-7. Epub 2023 Jun 19. Lancet Respir Med. 2023. PMID: 37348523 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
