

Changes in Oesophageal Transit, Macro-Reflux Events, and Gastric Emptying Correlate with Improvements in Gastro-Intestinal Symptoms and Food Tolerance Early Post Sleeve Gastrectomy
- PMID: 37349670
- PMCID: PMC10345052
- DOI: 10.1007/s11695-023-06695-z
Changes in Oesophageal Transit, Macro-Reflux Events, and Gastric Emptying Correlate with Improvements in Gastro-Intestinal Symptoms and Food Tolerance Early Post Sleeve Gastrectomy
Abstract
Purpose: There are significant alterations in gastro-intestinal function, food tolerance, and symptoms following sleeve gastrectomy (SG). These substantially change over the first year, but it is unclear what the underlying physiological basis for these changes is. We examined changes in oesophageal transit and gastric emptying and how these correlate with changes in gastro-intestinal symptoms and food tolerance.
Material and methods: Post-SG patients undertook protocolised nuclear scintigraphy imaging along with a clinical questionnaire at 6 weeks, 6 months, and 12 months.
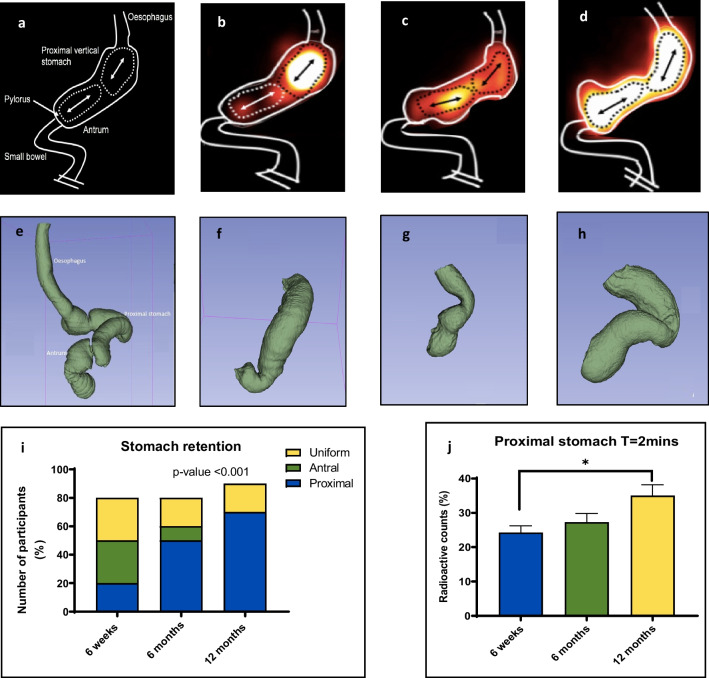
Results: Thirteen patients were studied: mean age (44.8 ± 8.5 years), 76.9% females, pre-operative BMI (46.9 ± 6.7 kg/m2). Post-operative %TWL was 11.9 ± 5.1% (6 weeks) and 32.2 ± 10.1% (12 months), p-value < 0.0001. There was a substantial increase of meal within the proximal stomach; 22.3% (IQR 12%) (6 weeks) vs. 34.2% (IQR 19.7%) (12 months), p = 0.038. Hyper-accelerated transit into the small bowel decreased from 6 weeks 49.6% (IQR 10.8%) to 42.7% (IQR 20.5%) 12 months, p = 0.022. Gastric emptying half-time increased from 6 weeks 19 (IQR 8.5) to 12 months 27 (IQR 11.5) min, p = 0.027. The incidence of deglutitive reflux of semi-solids decreased over time; 46.2% (6 weeks) vs. 18.2% (12 months), p-value < 0.0001. Reflux score of 10.6 ± 7.6 at 6 weeks vs. 3.5 ± 4.4 at 12 months, (p = 0.049) and regurgitation score of 9.9 ± 3.3 at 6 weeks vs. 6.5 ± 1.7, p = 0.021 significantly reduced.
Conclusions: These data demonstrate that there is an increase in the capacity of the proximal gastric sleeve to accommodate substrate over the first year. Gastric emptying remains rapid but reduce over time, correlating with improved food tolerance and reduced reflux symptoms. This is likely the physiological basis for the changes in symptoms and food tolerance observed early post-SG.
Keywords: Bariatric outcome; Bariatric surgery mechanism; Clinical trial; Food tolerance; Gastric emptying; Gastrointestinal symptoms; Nuclear scintigraphy; Physiology; Reflux; Sleeve.
© 2023. The Author(s).
Conflict of interest statement
Anagi C Wickremasinghe: was supported by an Australian Government Research Training Program (RTP) Scholarship. Yazmin Johari: no conflict of interest to declare. Helen Yue: no conflict of interest to declare. Cheryl Laurie: no conflict of interest to declare. Kalai Shaw: no conflict of interest to declare. Julie Playfair: no conflict of interest to declare. Paul Beech: no conflict of interest to declare. Geoffrey Hebbard: no conflict of interest to declare. Kenneth S Yap: no conflict of interest to declare. Wendy Brown: received grants from Johnson and Johnson, grants from Medtronic, grants from GORE, personal fees from GORE, grants from Applied Medical, grants from Apollo Endosurgery, grants and personal fees from Novo Nordisc, personal fees from Merck Sharpe and Dohme, outside the submitted work. Paul Burton: no conflict of interest to declare.
Figures

References
-
- Goldenshluger M, Goldenshluger A, Keinan-Boker L, Cohen MJ, Ben-Porat T, Gerasi H, et al. Postoperative outcomes, weight loss predictors, and late gastrointestinal symptoms following laparoscopic sleeve gastrectomy. J Gastrointest Surg. 2017;21(12):2009–2015. doi: 10.1007/s11605-017-3585-9. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
