

Assessing safe and personalised maternity and neonatal care through a pandemic: a case study of outcomes and experiences in two trusts in England using the ASPIRE COVID-19 framework
- PMID: 37349751
- PMCID: PMC10288742
- DOI: 10.1186/s12913-023-09669-0
Assessing safe and personalised maternity and neonatal care through a pandemic: a case study of outcomes and experiences in two trusts in England using the ASPIRE COVID-19 framework
Abstract
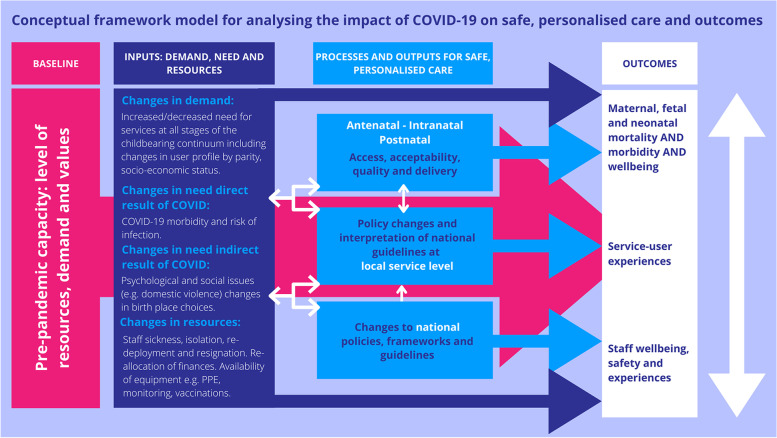
Background: The COVID-19 pandemic has resulted in profound and far-reaching impacts on maternal and newborn care and outcomes. As part of the ASPIRE COVID-19 project, we describe processes and outcome measures relating to safe and personalised maternity care in England which we map against a pre-developed ASPIRE framework to establish the potential impact of the COVID-19 pandemic for two UK trusts.
Methods: We undertook a mixed-methods system-wide case study using quantitative routinely collected data and qualitative data from two Trusts and their service users from 2019 to 2021 (start and completion dates varied by available data). We mapped findings to our prior ASPIRE conceptual framework that explains pathways for the impact of COVID-19 on safe and personalised care.
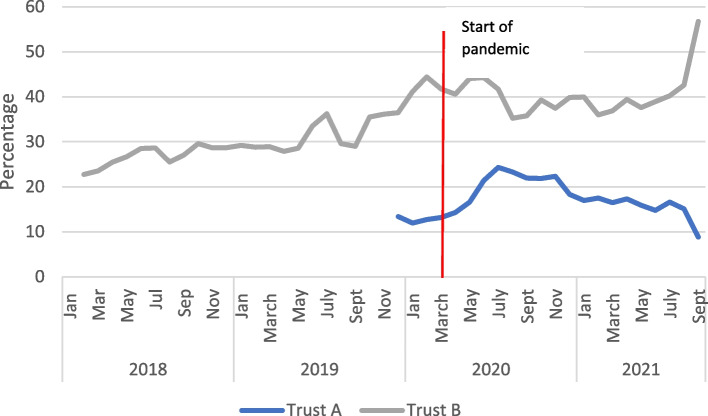
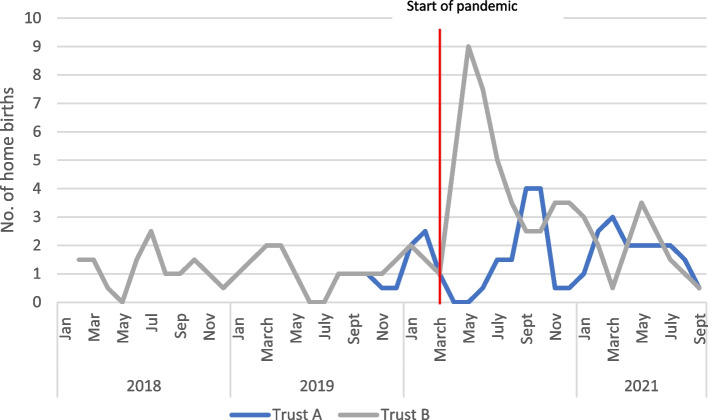
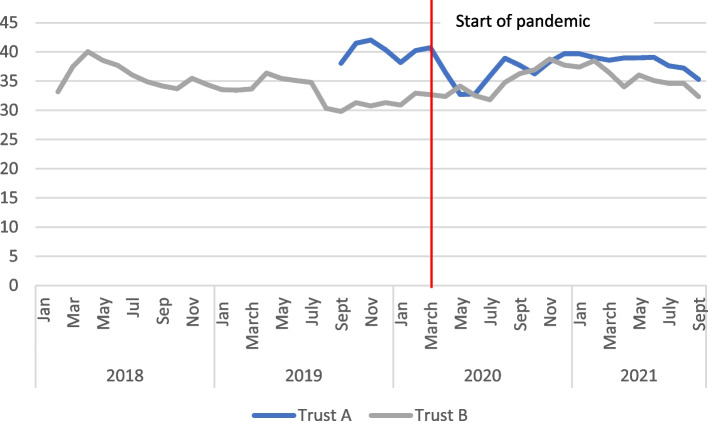
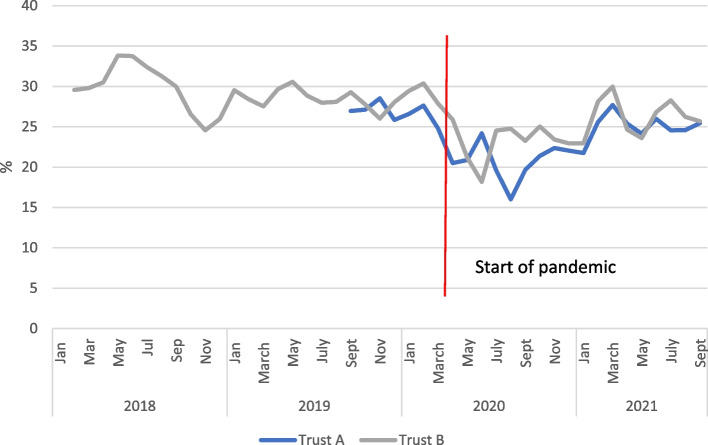
Results: The ASPIRE framework enabled us to develop a comprehensive, systems-level understanding of the impact of the pandemic on service delivery, user experience and staff wellbeing, and place it within the context of pre-existing challenges. Maternity services experienced some impacts on core service coverage, though not on Trust level clinical health outcomes (with the possible exception of readmissions in one Trust). Both users and staff found some pandemic-driven changes challenging such as remote or reduced antenatal and community postnatal contacts, and restrictions on companionship. Other key changes included an increased need for mental health support, changes in the availability and uptake of home birth services and changes in induction procedures. Many emergency adaptations persisted at the end of data collection. Differences between the trusts indicate complex change pathways. Staff reported some removal of bureaucracy, which allowed greater flexibility. During the first wave of COVID-19 staffing numbers increased, resolving some pre-pandemic shortages: however, by October 2021 they declined markedly. Trying to maintain the quality and availability of services had marked negative consequences for personnel. Timely routine clinical and staffing data were not always available and personalised care and user and staff experiences were poorly captured.
Conclusions: The COVID-19 crisis magnified pre-pandemic problems and in particular, poor staffing levels. Maintaining services took a significant toll on staff wellbeing. There is some evidence that these pressures are continuing. There was marked variation in Trust responses. Lack of accessible and timely data at Trust and national levels hampered rapid insights. The ASPIRE COVID-19 framework could be useful for modelling the impact of future crises on routine care.
Keywords: ASPIRE COVID-19; COVID-19; Case study; Crises; Maternal health services; Midwifery; Organisational evaluation framework.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Villar J, Ariff S, Gunier RB, Thiruvengadam R, Rauch S, Kholin A, et al. Maternal and neonatal morbidity and mortality among pregnant women with and without COVID-19 infection: the INTERCOVID multinational cohort study. JAMA Pediatr. 2021;175(8):817–826. doi: 10.1001/jamapediatrics.2021.1050. - DOI - PMC - PubMed
-
- Aranda Z, Binde T, Tashman K, Tadikonda A, Mawindo B, Maweu D, et al. Disruptions in maternal health service use during the COVID-19 pandemic in 2020: experiences from 37 health facilities in low-income and middle-income countries. BMJ Glob Health. 2022;7(1):7247. doi: 10.1136/bmjgh-2021-007247. - DOI - PMC - PubMed
-
- Jardine J, Relph S, Magee LA, von Dadelszen P, Morris E, Ross-Davie M, et al. Maternity services in the UK during the coronavirus disease 2019 pandemic: a national survey of modifications to standard care. Cited 2021 Jul 26. Available from: https://vimeo.com/rcog/authorinsights16547. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
