

Effect of a low versus intermediate tidal volume strategy on pulmonary complications in patients at risk of acute respiratory distress syndrome-a randomized clinical trial
- PMID: 37351068
- PMCID: PMC10282840
- DOI: 10.3389/fmed.2023.1172434
Effect of a low versus intermediate tidal volume strategy on pulmonary complications in patients at risk of acute respiratory distress syndrome-a randomized clinical trial
Abstract
Introduction: There is no consensus on whether invasive ventilation should use low tidal volumes (VT) to prevent lung complications in patients at risk of acute respiratory distress syndrome (ARDS). The purpose of this study is to determine if a low VT strategy is more effective than an intermediate VT strategy in preventing pulmonary complications.
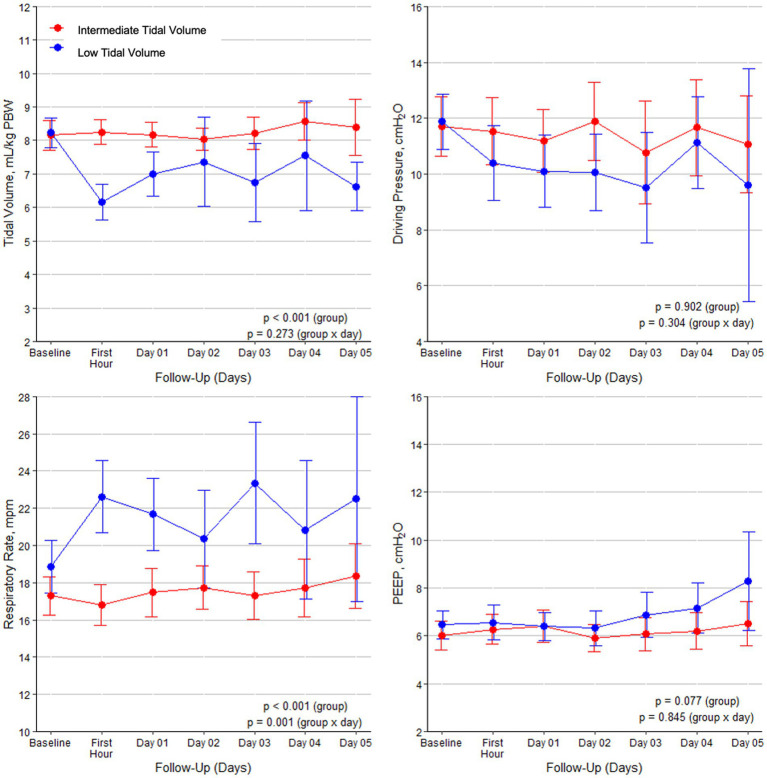
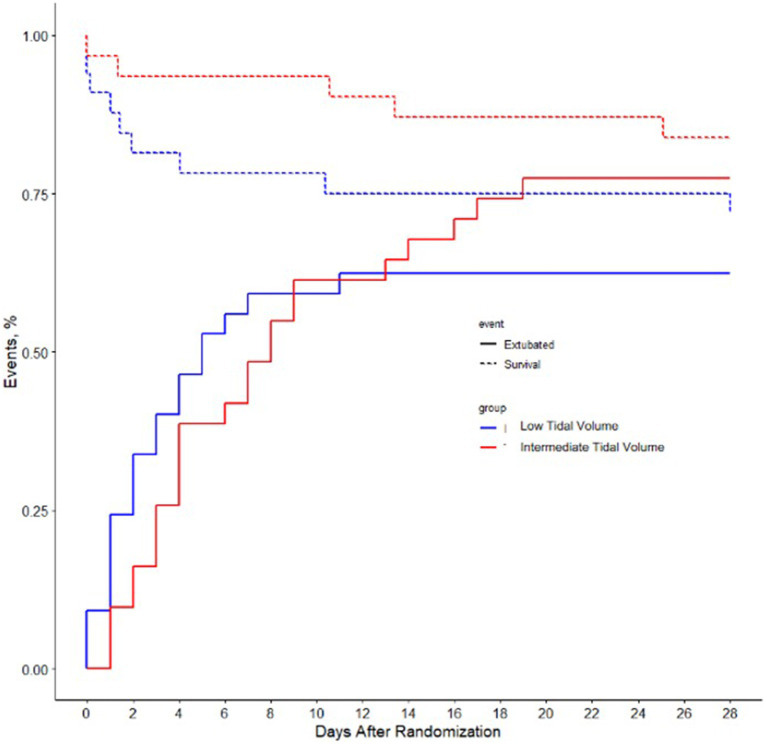
Methods: A randomized clinical trial was conducted in invasively ventilated patients with a lung injury prediction score (LIPS) of >4 performed in the intensive care units of 10 hospitals in Spain and one in the United States of America (USA) from 3 November 2014 to 30 August 2016. Patients were randomized to invasive ventilation using low VT (≤ 6 mL/kg predicted body weight, PBW) (N = 50) or intermediate VT (> 8 mL/kg PBW) (N = 48). The primary endpoint was the development of ARDS during the first 7 days after the initiation of invasive ventilation. Secondary endpoints included the development of pneumonia and severe atelectases; the length of intensive care unit (ICU) and hospital stay; and ICU, hospital, 28- and 90-day mortality.
Results: In total, 98 patients [67.3% male], with a median age of 65.5 years [interquartile range 55-73], were enrolled until the study was prematurely stopped because of slow recruitment and loss of equipoise caused by recent study reports. On day 7, five (11.9%) patients in the low VT group and four (9.1%) patients in the intermediate VT group had developed ARDS (risk ratio, 1.16 [95% CI, 0.62-2.17]; p = 0.735). The incidence of pneumonia and severe atelectasis was also not different between the two groups. The use of a low VT strategy did neither affect the length of ICU and hospital stay nor mortality rates.
Conclusions: In patients at risk for ARDS, a low VT strategy did not result in a lower incidence of ARDS than an intermediate VT strategy.Clinical Trial Registration: ClinicalTrials.gov, identifier NCT02070666.
Keywords: ARDS; critical care; intensive care; lung protection; mechanical ventilation; mortality; tidal volume.
Copyright © 2023 de Haro, Neto, Gomà, González, Ortega, Forteza, Frutos-Vivar, García, Simonis, Gordo-Vidal, Suarez, Schultz and Artigas.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. (2000) 342:1301–8. doi: 10.1056/NEJM200005043421801, PMID: - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical