

Long-term outcomes from the UK Biobank on the impact of coffee on cardiovascular disease, arrhythmias, and mortality: Does the future hold coffee prescriptions?
- PMID: 37351100
- PMCID: PMC10282813
- DOI: 10.21542/gcsp.2023.13
Long-term outcomes from the UK Biobank on the impact of coffee on cardiovascular disease, arrhythmias, and mortality: Does the future hold coffee prescriptions?
Abstract
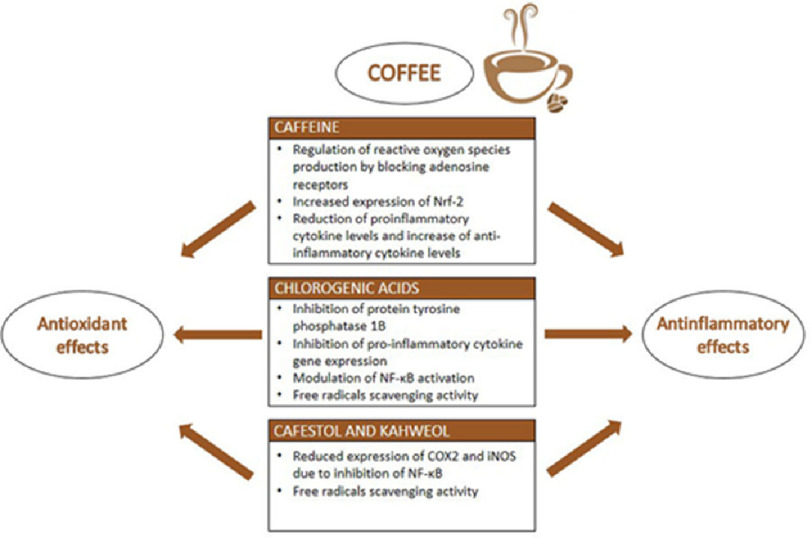
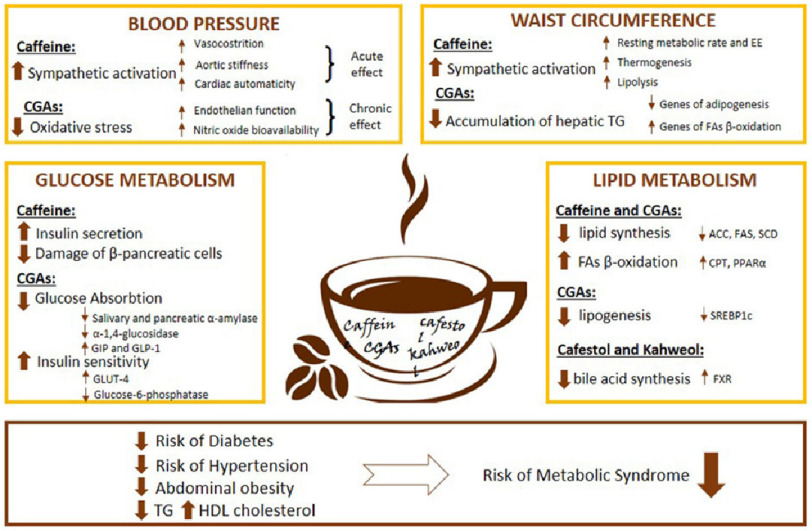
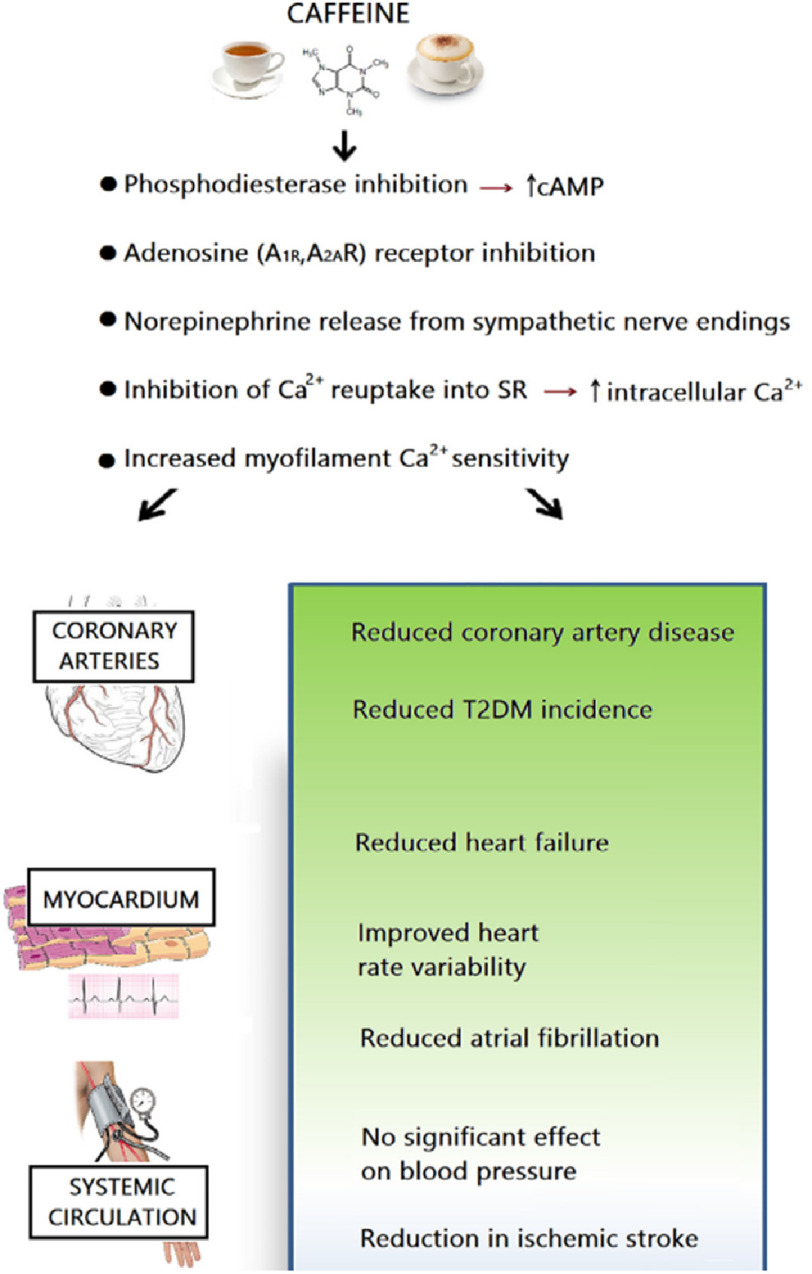
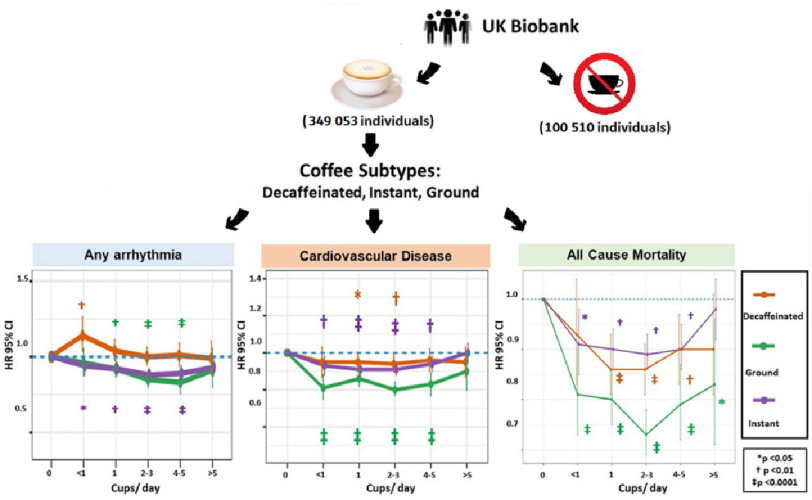
Introduction: Coffee is a popular beverage and the most used psychostimulant worldwide. Habitual coffee consumption has been linked to a growing list of health benefits; however, coffee consumption has been a source of longstanding debate. Recent observational studies have challenged the misconception of caffeine and reported the safety and beneficial effects of coffee intake on a range of cardiovascular (CV) conditions, including coronary artery disease, arrhythmias, heart failure, and stroke, leading to a decreased risk of CVD, all-cause and CVD mortality, and being associated with favorable CV outcomes. However, the mechanisms underlying the protective effects of caffeine remain speculative, and there is a lack of dedicated studies aimed at addressing the impact of different coffee subtypes on clinical outcomes such as CVD, arrhythmia, and mortality. Study and Results: The study included 449,563 UK Biobank participants, free of cardiovascular problems at enrollment (median age 58 years; 55.3% females). The median follow-up time was 12.5 years. Drinking 4 to 5 cups/day of ground (HR 0.83; 95% CI [0.76-0.91]; P < .0001) or 2 to 3 cups/day of instant (HR, 0.88; 95% CI [0.85-0.92]; P < .0001) coffee (but not decaffeinated coffee) was associated with a significant reduction in incident arrhythmia, including AF. Habitual coffee intake of up to 5 cups/day was associated with significant reductions in the risk of incident CVD, CHD (HR 0.89, CI [0.86-0.91], P < 0.0001), CCF (HR 0.83, CI [0.79-0.87], P < 0.0001), and ischemic stroke (HR 0.84, CI [0.78-0.90], P < 0.0001). Coffee consumption led to significant reductions in all-cause mortality (HR 0.86, CI [0.83-0.89], P < 0.0001) and CV mortality (HR 0.82, CI [0.74-0.90], P < 0.0001). Consumption of ground coffee at all levels significantly reduced the risk of all-cause and CV mortality. There was no significant difference in the incidence of CVD among all intake categories or across all coffee subtypes.
Lessons learned: The results from the UK Biobank indicate that mild-to-moderate consumption of all types of coffee is linked to improved CV outcomes and a lower risk of cardiovascular disease and death, with caffeinated coffee significantly reducing the risk of arrhythmias, including AF. Daily coffee intake should not be discouraged by physicians, even in the presence of a newly developed cardiovascular disease. Whether coffee will be prescribed in the future to prevent CVD and improve cardiovascular health depends on further evaluation of the physiological mechanisms and elucidation of the specific protective effects of coffee consumption.
Copyright ©2023 The Author(s).
Figures
Similar articles
-
The impact of coffee subtypes on incident cardiovascular disease, arrhythmias, and mortality: long-term outcomes from the UK Biobank.Eur J Prev Cardiol. 2022 Dec 7;29(17):2240-2249. doi: 10.1093/eurjpc/zwac189. Eur J Prev Cardiol. 2022. PMID: 36162818
-
Effects of habitual coffee consumption on cardiometabolic disease, cardiovascular health, and all-cause mortality.J Am Coll Cardiol. 2013 Sep 17;62(12):1043-1051. doi: 10.1016/j.jacc.2013.06.035. Epub 2013 Jul 17. J Am Coll Cardiol. 2013. PMID: 23871889 Review.
-
Light to moderate coffee consumption is associated with lower risk of death: a UK Biobank study.Eur J Prev Cardiol. 2022 May 6;29(6):982-991. doi: 10.1093/eurjpc/zwac008. Eur J Prev Cardiol. 2022. PMID: 35048949
-
Coffee Consumption and Incidence of Cardiovascular and Microvascular Diseases in Never-Smoking Adults with Type 2 Diabetes Mellitus.Nutrients. 2023 Sep 8;15(18):3910. doi: 10.3390/nu15183910. Nutrients. 2023. PMID: 37764694 Free PMC article.
-
Coffee and tea consumption and cardiovascular disease and all-cause and cause-specific mortality in individuals with diabetes mellitus: a meta-analysis of prospective observational studies.Front Nutr. 2025 Jun 2;12:1570644. doi: 10.3389/fnut.2025.1570644. eCollection 2025. Front Nutr. 2025. PMID: 40525136 Free PMC article.
Cited by
-
Sex Related Differences in the Complex Relationship between Coffee, Caffeine and Atrial Fibrillation.Nutrients. 2023 Jul 25;15(15):3299. doi: 10.3390/nu15153299. Nutrients. 2023. PMID: 37571236 Free PMC article. Review.
-
Heartbreakers: Decoding the Molecular Dynamics of Stimulants Abuse on the Cardiovascular System.Discoveries (Craiova). 2025 May 10;13(1):e207. doi: 10.15190/d.2025.6. eCollection 2025 Apr-Jun. Discoveries (Craiova). 2025. PMID: 40656765 Free PMC article. Review.
-
The Role of Xenobiotic Caffeine on Cardiovascular Health: Promises and Challenges.J Xenobiot. 2025 Mar 31;15(2):51. doi: 10.3390/jox15020051. J Xenobiot. 2025. PMID: 40278156 Free PMC article. Review.
-
Tea and coffee consumption and risk of acute stroke: The INTERSTROKE Study.Int J Stroke. 2024 Oct;19(9):1053-1063. doi: 10.1177/17474930241264685. Epub 2024 Jul 31. Int J Stroke. 2024. PMID: 38887998 Free PMC article.
References
-
- Setiawan VW, Wilkens LR, Lu SC, Hernandez BY, le Marchand L, Henderson BE. Association of coffee intake with reduced incidence of liver cancer and death from chronic liver disease in the US multiethnic cohort. Gastroenterology. 2015;148(1):118–125. doi: 10.1053/j.gastro.2014.10.005. doi: - DOI - PMC - PubMed
-
- Bravi F, Tavani A, Bosetti C, Boffetta P, la Vecchia C. Coffee and the risk of hepatocellular carcinoma and chronic liver disease: a systematic review and meta-analysis of prospective studies. European Journal of Cancer Prevention. 2017;26(5):368–377. doi: 10.1097/CEJ.0000000000000252. doi: - DOI - PubMed
LinkOut - more resources
Full Text Sources