

Large, multifocal or portal vein-invading hepatocellular carcinoma (HCC) downstaged by Y90 using personalized dosimetry: safety, pathological results and outcomes after surgery
- PMID: 37351147
- PMCID: PMC10282681
- DOI: 10.21037/hbsn-22-184
Large, multifocal or portal vein-invading hepatocellular carcinoma (HCC) downstaged by Y90 using personalized dosimetry: safety, pathological results and outcomes after surgery
Abstract
Background: Transarterial radioembolization (TARE) has recently been recognized as a bridging/downstaging therapy to surgery for early hepatocellular carcinomas (HCCs) with high rates of complete pathological necrosis (CPN) on liver explants. In patients with portal vein tumoral thrombus (PVTT), multifocal or large tumors, TARE has mainly a palliative role and surgery remains controversial in this poor-prognosis population. Personalized dosimetry recently proved to outperform standard dosimetry used in prior negative Y90 randomized-controlled trials.
Methods: In this retrospective study, we evaluated safety, radiological and pathological response and outcomes in HCC patients with PVTT, multifocal or large tumors, who underwent surgery after downstaging using TARE with Y90-loaded glass microspheres with personalized dosimetry.
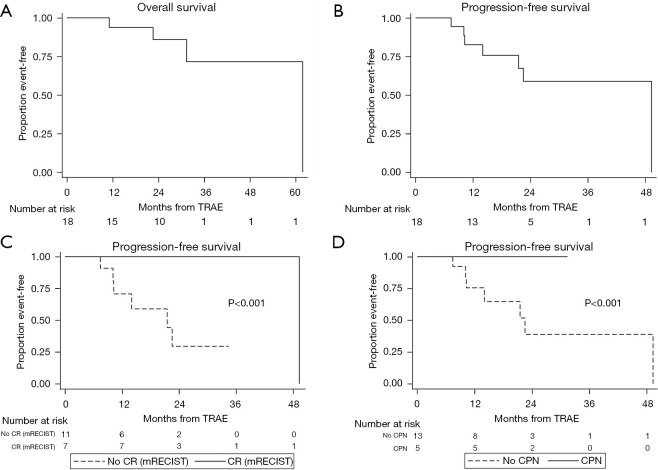
Results: Between December 2015 and October 2021, 18 unresectable patients (14/18 with PVTT) had surgery (16 resections, 2 liver transplantations) 6.2 months (range, 2-14.6 months) after a single Y90 treatment. No 90-day mortality was reported. Objective modified response criteria in solid tumors (mRECIST) response were noted in all but one patient. Complete and extensive (50-99%) necrosis was observed in 36% and 45% of tumors, respectively. The post-treatment tumor-absorbed dose significantly differed depending on the extent of pathological necrosis (P=0.045). Median overall survival and progression-free survival (PFS) were respectively of 61.8 months [95% CI: 31.4 months-not reached (NR)] and 49.3 months (95% CI: 14 months-NR). PFS was longer in patients with complete imaging response [median NR (none recurred or died) vs. 21.5 months (95% CI: 10.1 months-NR), P<0.001] and in those with complete pathological response [median NR vs. 22.5 months (95% CI: 10.1 months-NR), P<0.001].
Conclusions: Y90 TARE using personalized dosimetry can provide high rates of imaging and pathological response in patients with PVTT, large or multifocal HCC. Subsequent surgery is safe and leads to outcomes far exceeding expectations in an otherwise poor prognosis population with no chance for cure.
Trial registration: Clinical trial number: NCT05045573.
Keywords: Selective internal radiation therapy; hepatocellular carcinoma (HCC); liver cancer; resection; transplantation.
2023 Hepatobiliary Surgery and Nutrition. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://hbsn.amegroups.com/article/view/10.21037/hbsn-22-184/coif). FP and BG serve as unpaid editorial board members of Hepatobiliary Surgery and Nutrition. CA and BG report receiving consulting fees from Boston scientific as consultants, and receiving payment from Boston scientific for presentations. The other authors have no conflicts of interest to declare.
Figures



References
Associated data
LinkOut - more resources
Full Text Sources
Medical