

Health care impact of implementing a clinical pathway for acute care of pediatric concussion: a stepped wedge, cluster randomised trial
- PMID: 37351798
- PMCID: PMC10333406
- DOI: 10.1007/s43678-023-00530-1
Health care impact of implementing a clinical pathway for acute care of pediatric concussion: a stepped wedge, cluster randomised trial
Abstract
Objectives: To test the effects of actively implementing a clinical pathway for acute care of pediatric concussion on health care utilization and costs.
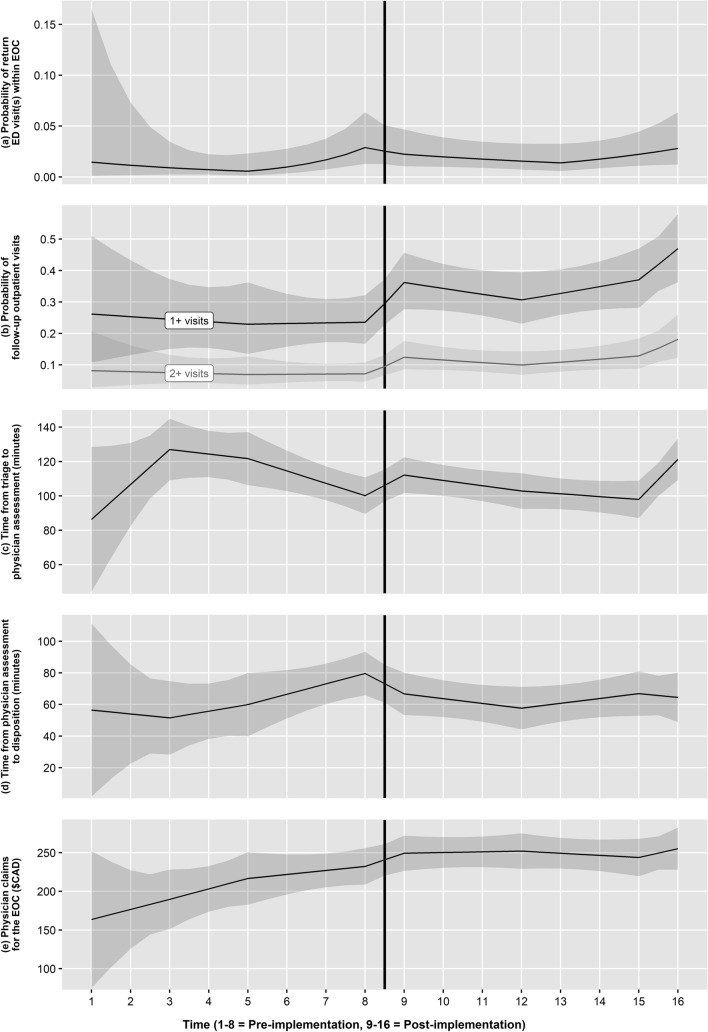
Methods: Stepped wedge, cluster randomized trial of a clinical pathway, conducted in 5 emergency departments (ED) in Alberta, Canada from February 1 to November 30, 2019. The clinical pathway emphasized standardized assessment of risk for persistent symptoms, provision of consistent information to patients and families, and referral for outpatient follow-up. De-identified administrative data measured 6 outcomes: ED return visits; outpatient follow-up visits; length of ED stay, including total time, time from triage to physician initial assessment, and time from physician initial assessment to disposition; and total physician claims in an episode of care.
Results: A total of 2878 unique patients (1164 female, 1713 male) aged 5-17 years (median 11.00, IQR 8, 14) met case criteria. They completed 3009 visits to the 5 sites and 781 follow-up visits to outpatient care, constituting 2910 episodes of care. Implementation did not alter the likelihood of an ED return visit (OR 0.77, 95% CI 0.39, 1.52), but increased the likelihood of outpatient follow-up visits (OR 1.84, 95% CI 1.19, 2.85). Total length of ED stay was unchanged, but time from physician initial assessment to disposition decreased significantly (mean change - 23.76 min, 95% CI - 37.99, - 9.52). Total physician claims increased significantly at only 1 of 5 sites.
Conclusions: Implementation of a clinical pathway in the ED increased outpatient follow-up and reduced the time from physician initial assessment to disposition, without increasing physician costs. Implementation of a clinical pathway can align acute care of pediatric concussion more closely with existing clinical practice guidelines while making care more efficient.
Trial registration: ClinicalTrials.gov NCT05095012.
Abstrait: OBJECTIFS: Mettre à l’essai les effets de la mise en œuvre active d’une voie clinique pour le traitement aigu des commotions cérébrales chez les enfants sur l’utilisation et les coûts des soins de santé. MéTHODES: Essai randomisé en grappes d’une voie clinique, échelonné, mené dans cinq services d’urgence en Alberta, au Canada, du 1 février au 30 novembre 2019. Le cheminement clinique mettait l’accent sur l’évaluation normalisée du risque de symptômes persistants, la fourniture de renseignements uniformes aux patients et aux familles, et l’aiguillage vers un suivi externe. Les données administratives dépersonnalisées ont permis de mesurer six résultats : visites de retour à l’urgence; visites de suivi en clinique externe; durée du séjour à l’urgence, y compris le temps total. le temps entre le triage et l’évaluation initiale du médecin, et le temps entre l’évaluation initiale du médecin et la décision; et le nombre total de demandes de remboursement du médecin dans un épisode de soins. RéSULTATS: Un total de 2878 patients uniques (1164 femmes, 1713 hommes) âgés de 5 à 17 ans (médiane 11,00, IQR 8, 14) répondaient aux critères de cas. Ils ont effectué 3009 visites aux 5 sites et 781 visites de suivi aux soins ambulatoires, ce qui représente 2910 épisodes de soins. La mise en œuvre n’a pas modifié la probabilité d’une visite de retour à l’urgence (RC 0,77, IC à 95 %, 0,39, 1,52), mais a augmenté la probabilité de visites de suivi en clinique externe (RC 1,84, IC à 95 %, 1,19, 2,85). La durée totale du séjour à l’urgence est demeurée inchangée, mais le temps écoulé entre l’évaluation initiale du médecin et la décision a diminué considérablement (changement moyen : -23,76 minutes, IC à 95 %, -37,99, -9,52). Le nombre total de demandes de règlement de médecins a augmenté de façon significative à seulement 1 site sur 5.
Conclusions: La mise en œuvre d’un cheminement clinique à l’urgence a augmenté le suivi des patients externes et réduit le temps entre l’évaluation initiale du médecin et son élimination, sans augmenter les coûts des médecins. La mise en œuvre d’un cheminement clinique peut harmoniser davantage les soins de courte durée en cas de commotion cérébrale pédiatrique avec les lignes directrices de pratique clinique existantes tout en rendant les soins plus efficaces. ENREGISTREMENT D’ESSAI: ClinicalTrials.gov NCT05095012.
Keywords: Clinical pathway; Pediatric; Traumatic brain injury; Utilization.
© 2023. The Author(s).
Conflict of interest statement
Keith Yeates is supported by the Ronald and Irene Ward Chair in Pediatric Brain Injury from the Alberta Children’s Hospital Foundation. Karen Barlow is supported by the Paul Hopkins Chair in Pediatric Brain Injury Rehabilitation from the Queensland Children’s Hospital Foundation and the Motor Accident Insurance Commission. Roger Zemek is supported by a Clinical Research Chair in Pediatric Concussion from University of Ottawa, and is the co-founder, Scientific Director and a minority shareholder in 360 Concussion Care, an interdisciplinary concussion clinic. Jennifer Zwicker is supported by the Canada Research Chair in Disability Policy for Children and Youth.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
