

Parathyroidectomy and survival in a cohort of Italian dialysis patients: results of a multicenter, observational, prospective study
- PMID: 37351832
- PMCID: PMC10543527
- DOI: 10.1007/s40620-023-01658-0
Parathyroidectomy and survival in a cohort of Italian dialysis patients: results of a multicenter, observational, prospective study
Abstract
Background: Severe secondary hyperparathyroidism (SHPT) is associated with mortality in end stage kidney disease (ESKD). Parathyroidectomy (PTX) becomes necessary when medical therapy fails, thus highlighting the interest to compare biochemical and clinical outcomes of patients receiving either medical treatment or surgery.
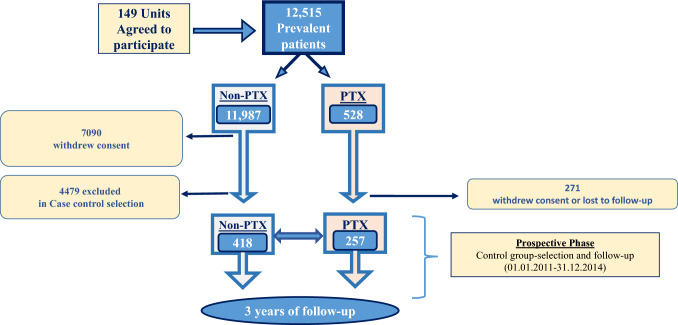
Methods: We aimed to compare overall survival and biochemical control of hemodialysis patients with severe hyperparathyroidism, treated by surgery or medical therapy followed-up for 36 months. Inclusion criteria were age older than 18 years, renal failure requiring dialysis treatment (hemodialysis or peritoneal dialysis) and ability to sign the consent form. A control group of 418 patients treated in the same centers, who did not undergo parathyroidectomy was selected after matching for age, sex, and dialysis vintage.
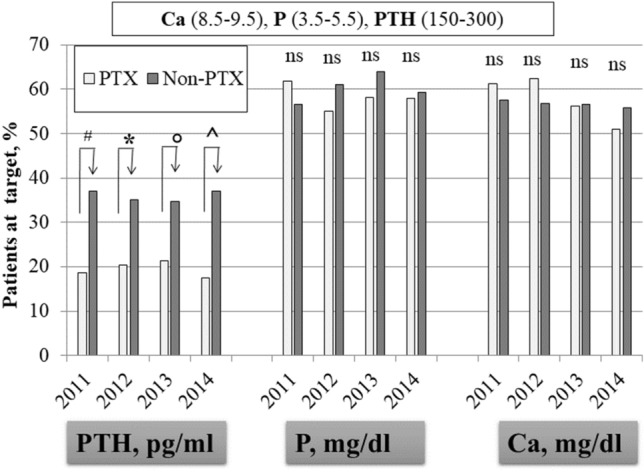
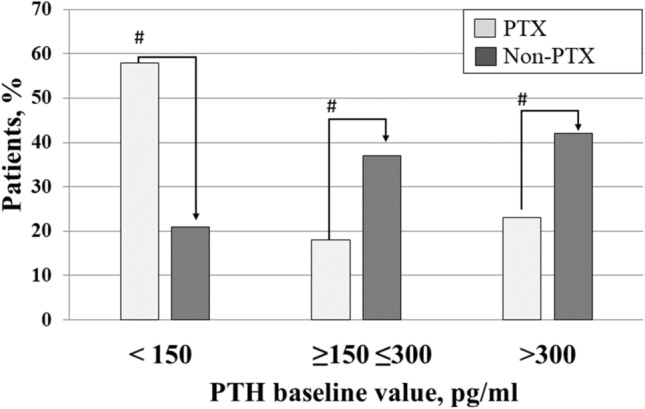
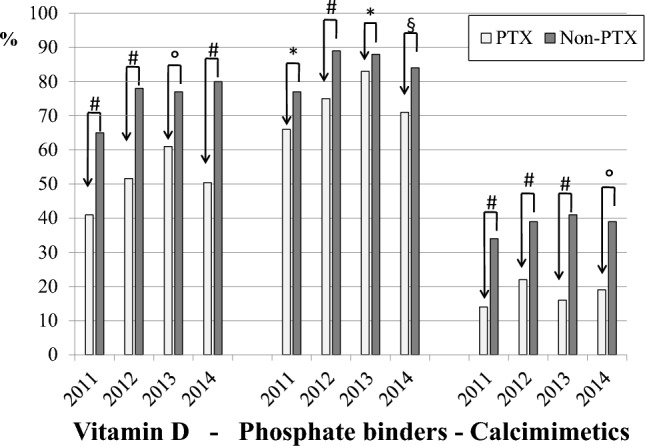
Results: From 82 Dialysis units in Italy, we prospectively collected data of 257 prevalent patients who underwent parathyroidectomy (age 58.2 ± 12.8 years; M/F: 44%/56%, dialysis vintage: 15.5 ± 8.4 years) and of 418 control patients who did not undergo parathyroidectomy (age 60.3 ± 14.4 years; M/F 44%/56%; dialysis vintage 11.2 ± 7.6 y). The survival rate was higher in the group that underwent parathyroidectomy (Kaplan-Meier log rank test = 0.002). Univariable analysis (HR 0.556, CI: 0.387-0.800, p = 0.002) and multivariable analysis (HR 0.671, CI:0.465-0.970, p = 0.034), identified parathyroidectomy as a protective factor of overall survival. The prevalence of patients at KDOQI targets for PTH was lower in patients who underwent parathyroidectomy compared to controls (PTX vs non-PTX: PTH < 150 pg/ml: 59% vs 21%, p = 0.001; PTH at target: 18% vs 37% p = 0.001; PTH > 300 pg/ml 23% vs 42% p = 0.001). The control group received more intensive medical treatment with higher prevalence of vitamin D (65% vs 41%, p = 0.0001), calcimimetics (34% vs 14%, p = 0.0001) and phosphate binders (77% vs 66%, p = 0.002).
Conclusions: Our data suggest that parathyroidectomy is associated with survival rate at 36 months, independently of biochemical control. Lower exposure to high PTH levels could represent an advantage in the long term.
Keywords: CKD-MBD; Hemodialysis; Mortality; Parathyroidectomy.
© 2023. The Author(s).
Conflict of interest statement
SM received honoraria for Congress presentations by Viforpharma and Amgen.
Figures

References
-
- Torres PA, De Broe M. Calcium-sensing receptor, calcimimetics, and cardiovascular calcifications in chronic kidney disease. KidneyInt. 2012;82:19–25. - PubMed
-
- London GM, Marty C, Marchais SJ, Guerin AP, Metivier F, de Vernejoul MC. Arterial calcifications and bone histomorphometry in end-stage renal disease. J Am SocNephrol. 2004;15(7):1943–1951. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
