

Association Between Anti-CD20 Therapies and COVID-19 Severity Among Patients With Relapsing-Remitting and Progressive Multiple Sclerosis
- PMID: 37351881
- PMCID: PMC10290250
- DOI: 10.1001/jamanetworkopen.2023.19766
Association Between Anti-CD20 Therapies and COVID-19 Severity Among Patients With Relapsing-Remitting and Progressive Multiple Sclerosis
Abstract
Importance: In patients with multiple sclerosis (MS), factors associated with severe COVID-19 include anti-CD20 therapies and neurologic disability, but it is still unclear whether these 2 variables are independently associated with severe COVID-19 or whether the association depends on MS clinical course.
Objective: To assess the association between anti-CD20 therapies and COVID-19 severity in patients with relapsing-remitting MS (RRMS) and progressive MS (PMS).
Design, setting, and participants: This multicenter, retrospective cohort study used data from the COVISEP study, which included patients with MS and COVID-19 from February 1, 2020, to June 30, 2022, at 46 French MS expert centers, general hospitals, and private neurology practices. Eligible patients with RRMS were those treated with high-efficacy MS therapy (ie, anti-CD20, fingolimod, or natalizumab), and eligible patients with PMS were those younger than 70 years with an Expanded Disability Status Scale (EDSS) score of 8 or lower. Patients were monitored from COVID-19 symptom onset until recovery or death.
Exposures: Current anti-CD20 therapy (ocrelizumab or rituximab).
Main outcomes and measures: The main outcome was severe COVID-19 (ie, hospitalization with any mode of oxygenation or death). All analyses were conducted separately in patients with RRMS and PMS using propensity score-weighted logistic regression. Subgroup analyses were performed according to COVID-19 vaccine status, sex, EDSS score, and age.
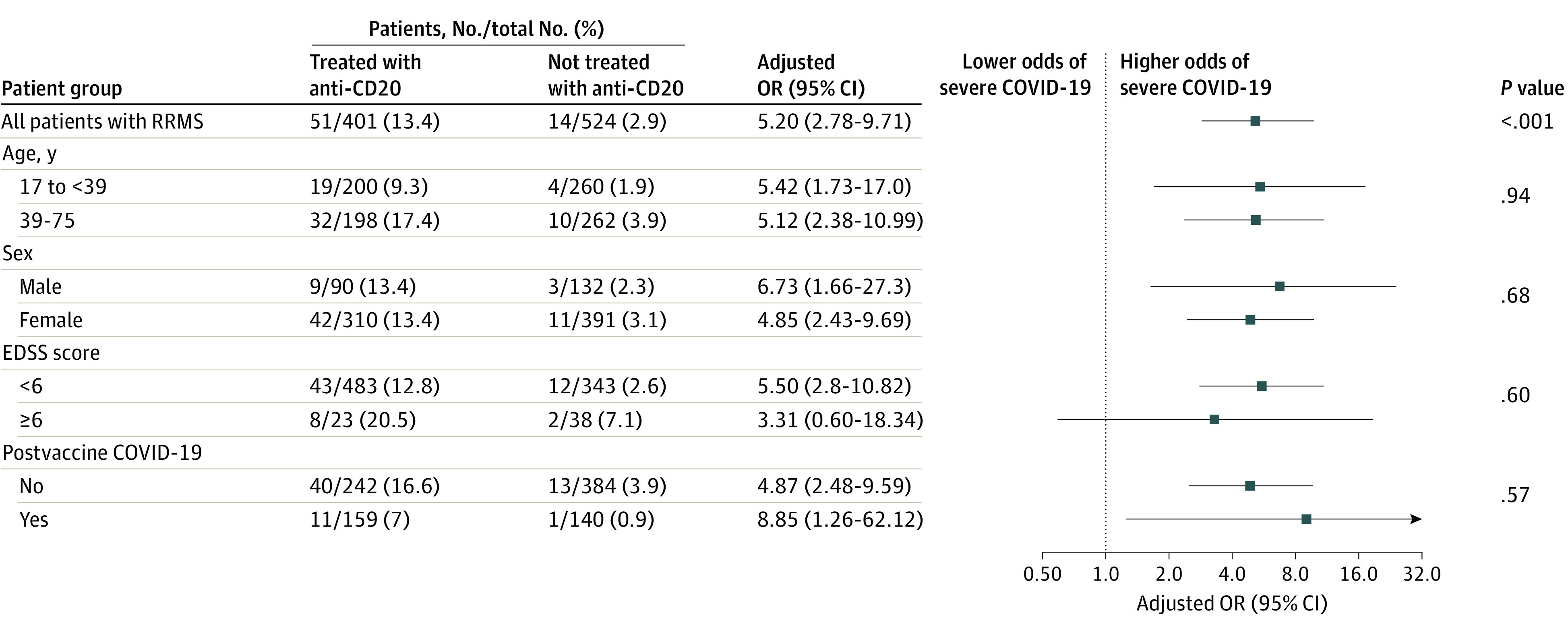
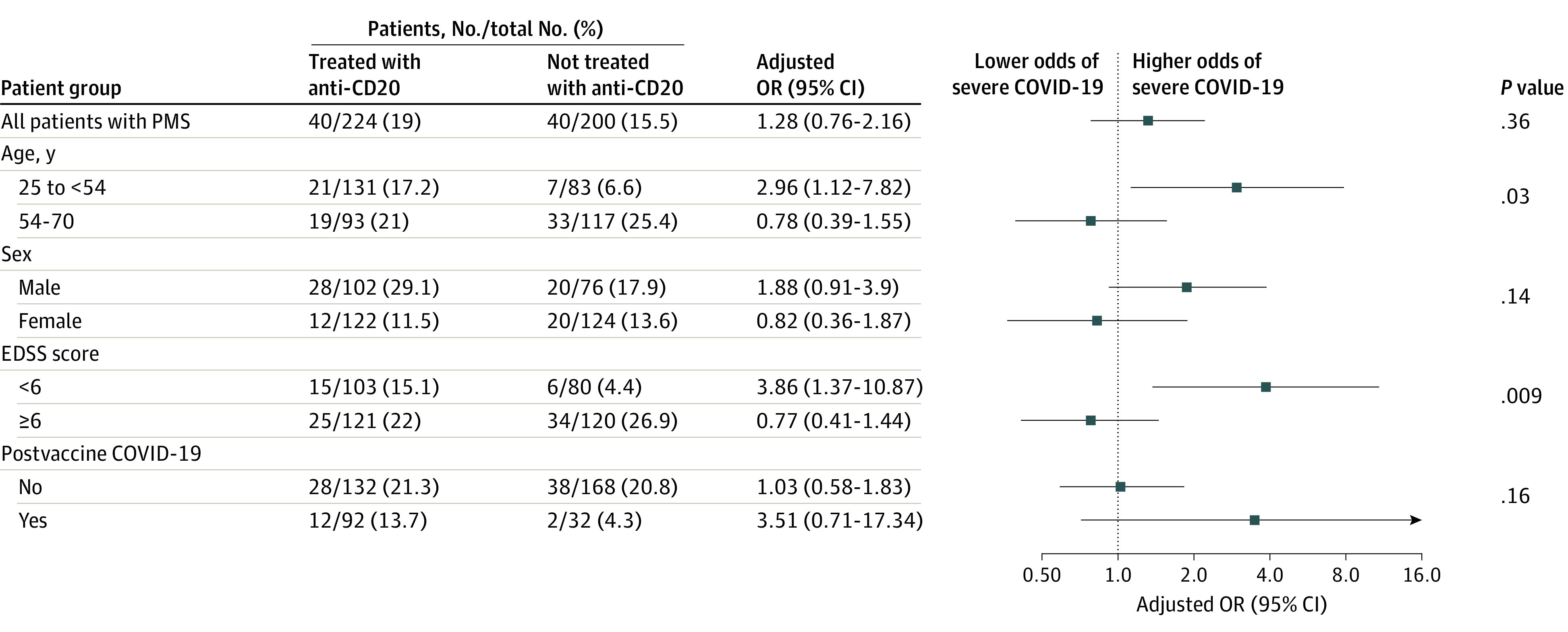
Results: A total of 1400 patients, 971 with RRMS (median age, 39.14 years [IQR, 31.38-46.80 years]; 737 [76.1%] female) and 429 with PMS (median age, 54.21 years [IQR, 48.42-60.14 years]; 250 [58.3%] female) were included in the study. A total of 418 patients with RRMS (43.0%) and 226 with PMS (52.7%) were treated with anti-CD20 therapies. In weighted analysis, 13.4% and 2.9% of patients with RRMS treated and not treated with anti-CD20 had severe COVID-19, respectively, and anti-CD20 treatment was associated with increased risk of severe COVID-19 (odds ratio [OR], 5.20; 95% CI, 2.78-9.71); this association persisted among vaccinated patients (7.0% vs 0.9%; OR, 8.85; 95% CI, 1.26-62.12). Among patients with PMS, 19.0% and 15.5% of patients treated and not treated with anti-CD20 had severe COVID-19, respectively, and there was no association between anti-CD20 treatment and severe COVID-19 (OR, 1.28; 95% CI, 0.76-2.16). In PMS subgroup analysis, anti-CD20 exposure interacted negatively with EDSS score (P = .009 for interaction) and age (P = .03 for interaction); anti-CD20 therapies were associated with risk of severe COVID-19 only in patients with less neurologic disability and younger patients with PMS.
Conclusions and relevance: In this cohort study, risk of severe COVID-19 was higher in patients with PMS than in those with RRMS. Use of anti-CD20 therapies was associated with an increased risk of severe COVID-19 among patients with RRMS. In patients with PMS, there was no association between anti-CD20 therapies and risk of severe COVID-19.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
