

Epidemiology of SARS-CoV-2 transmission and superspreading in Salt Lake County, Utah, March-May 2020
- PMID: 37352280
- PMCID: PMC10289415
- DOI: 10.1371/journal.pone.0275125
Epidemiology of SARS-CoV-2 transmission and superspreading in Salt Lake County, Utah, March-May 2020
Abstract
Background: Understanding the drivers of SARS-CoV-2 transmission can inform the development of interventions. We evaluated transmission identified by contact tracing investigations between March-May 2020 in Salt Lake County, Utah, to quantify the impact of this intervention and identify risk factors for transmission.
Methods: RT-PCR positive and untested symptomatic contacts were classified as confirmed and probable secondary case-patients, respectively. We compared the number of case-patients and close contacts generated by different groups, and used logistic regression to evaluate factors associated with transmission.
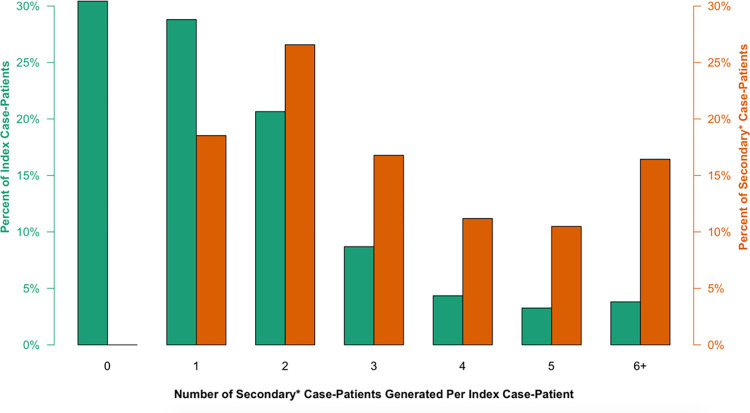
Results: Data were collected on 184 index case-patients and up to six generations of contacts. Of 1,499 close contacts, 374 (25%) were classified as secondary case-patients. Decreased transmission odds were observed for contacts aged <18 years (OR = 0.55 [95% CI: 0.38-0.79]), versus 18-44 years, and for workplace (OR = 0.36 [95% CI: 0.23-0.55]) and social (OR = 0.44 [95% CI: 0.28-0.66]) contacts, versus household contacts. Higher transmission odds were observed for case-patient's spouses than other household contacts (OR = 2.25 [95% CI: 1.52-3.35]). Compared to index case-patients identified in the community, secondary case-patients identified through contract-tracing generated significantly fewer close contacts and secondary case-patients of their own. Transmission was heterogeneous, with 41% of index case-patients generating 81% of directly-linked secondary case-patients.
Conclusions: Given sufficient resources and complementary public health measures, contact tracing can contain known chains of SARS-CoV-2 transmission. Transmission is associated with age and exposure setting, and can be highly variable, with a few infections generating a disproportionately high share of onward transmission.
Copyright: This is an open access article, free of all copyright, and may be freely reproduced, distributed, transmitted, modified, built upon, or otherwise used by anyone for any lawful purpose. The work is made available under the Creative Commons CC0 public domain dedication.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- CDC. Investigating a COVID-19 Case. Available from: https://www.cdc.gov/coronavirus/2019-ncov/php/contact-tracing/contact-tr....
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
