

Predictors of chronic thromboembolic pulmonary hypertension in patients with submassive pulmonary embolism treated with catheter-directed thrombolysis versus anticoagulation alone: A secondary analysis of the SUNSET sPE trial
- PMID: 37353154
- PMCID: PMC10630068
- DOI: 10.1016/j.jvsv.2023.06.003
Predictors of chronic thromboembolic pulmonary hypertension in patients with submassive pulmonary embolism treated with catheter-directed thrombolysis versus anticoagulation alone: A secondary analysis of the SUNSET sPE trial
Abstract
Objective: Chronic thromboembolic pulmonary hypertension (CTEPH) after pulmonary embolism (PE) is a morbid complication with suboptimal treatment. We aimed to evaluate the biomarker profile and functional outcomes in patients with submassive PE (sPE) treated with catheter-directed thrombolysis (CDT) compared with anticoagulation alone (ACA). We performed a secondary biomarker and survey analysis of the SUNSET sPE (standard vs ultrasound-assisted catheter thrombolysis for submassive pulmonary embolism) randomized trial comparing standard CDT to ultrasound-assisted thrombolysis in patients with sPE.
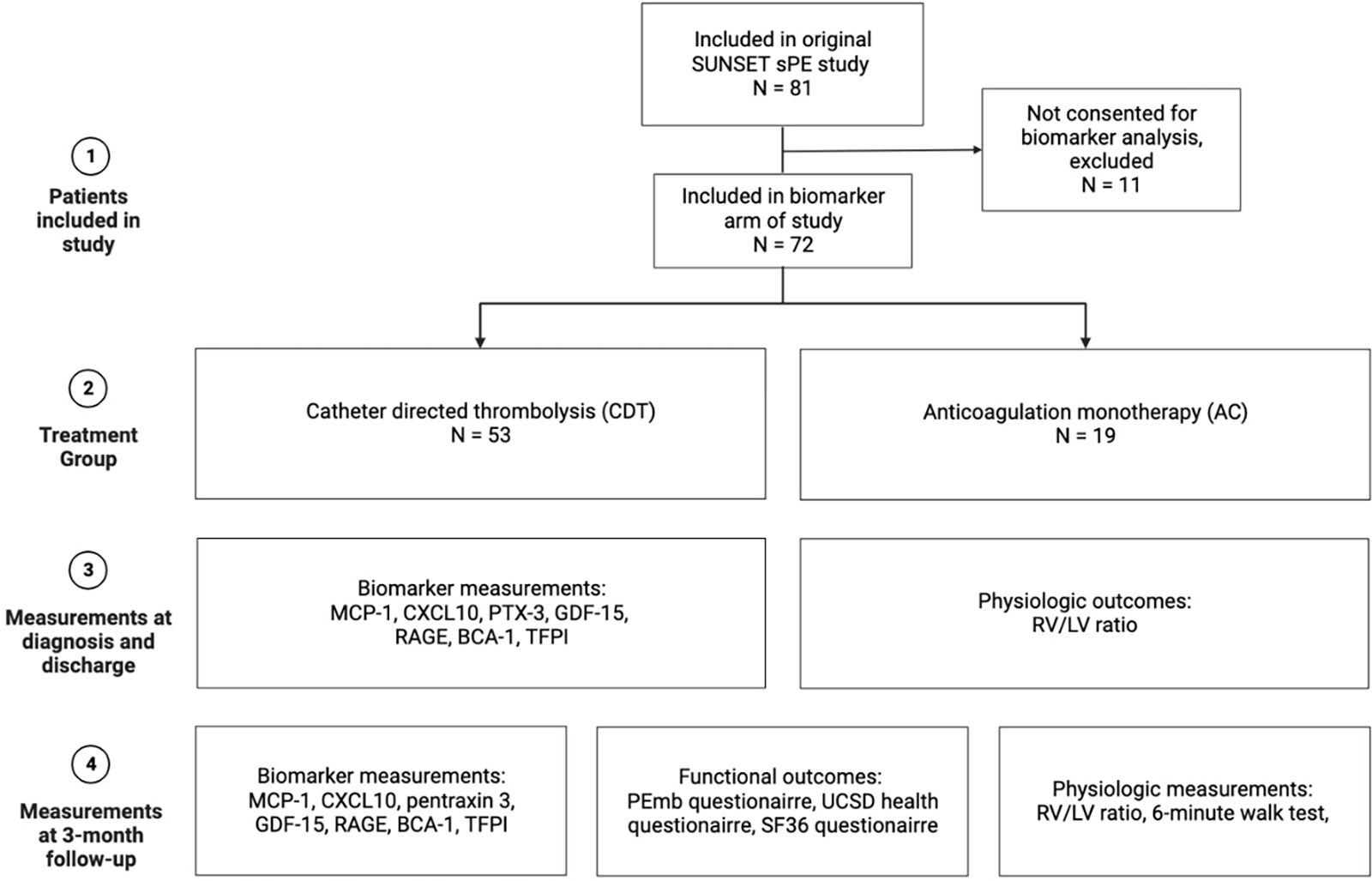
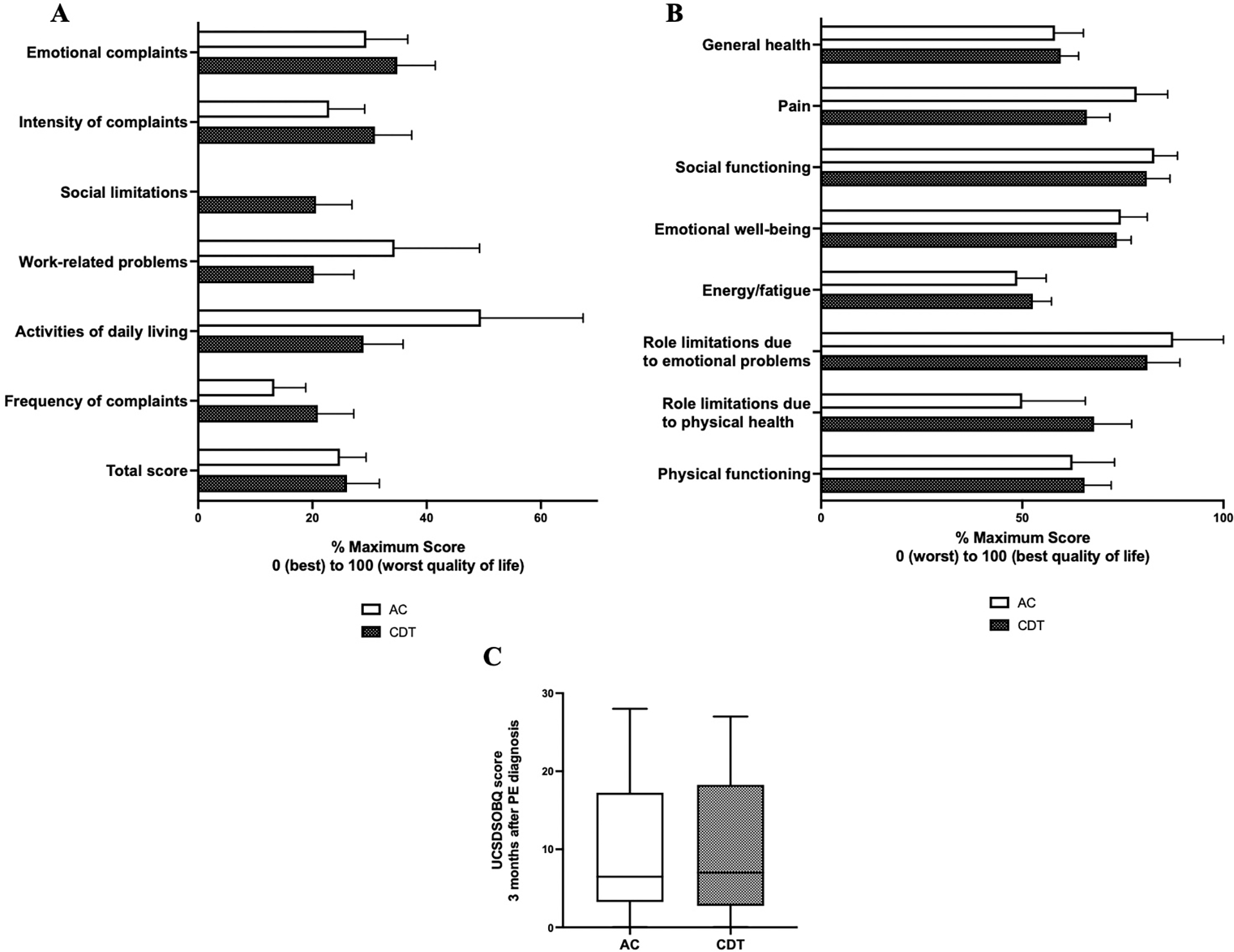
Methods: As a part of the SUNSET sPE study, patients who did not receive an intervention were enrolled in the medical (ACA) arm. The biomarkers associated with CTEPH in the literature (ie, CCL2, CXCL10, PTX3, GDF-15, RAGE, BCA-1, TFPI) were collected and measured using a multiplex assay at diagnosis, discharge, and 3-month follow-up. Patients underwent a 6-minute walk test and answered quality-of-life questionnaires (pulmonary embolism quality of life; University of California, San Diego, shortness of breath questionnaire; 36-item short-form survey) at 3 months after diagnosis. Comparisons were made using the Student t test. Nonparametric tests were used when the distributions were not normal. Significance was set at P ≤ .05.
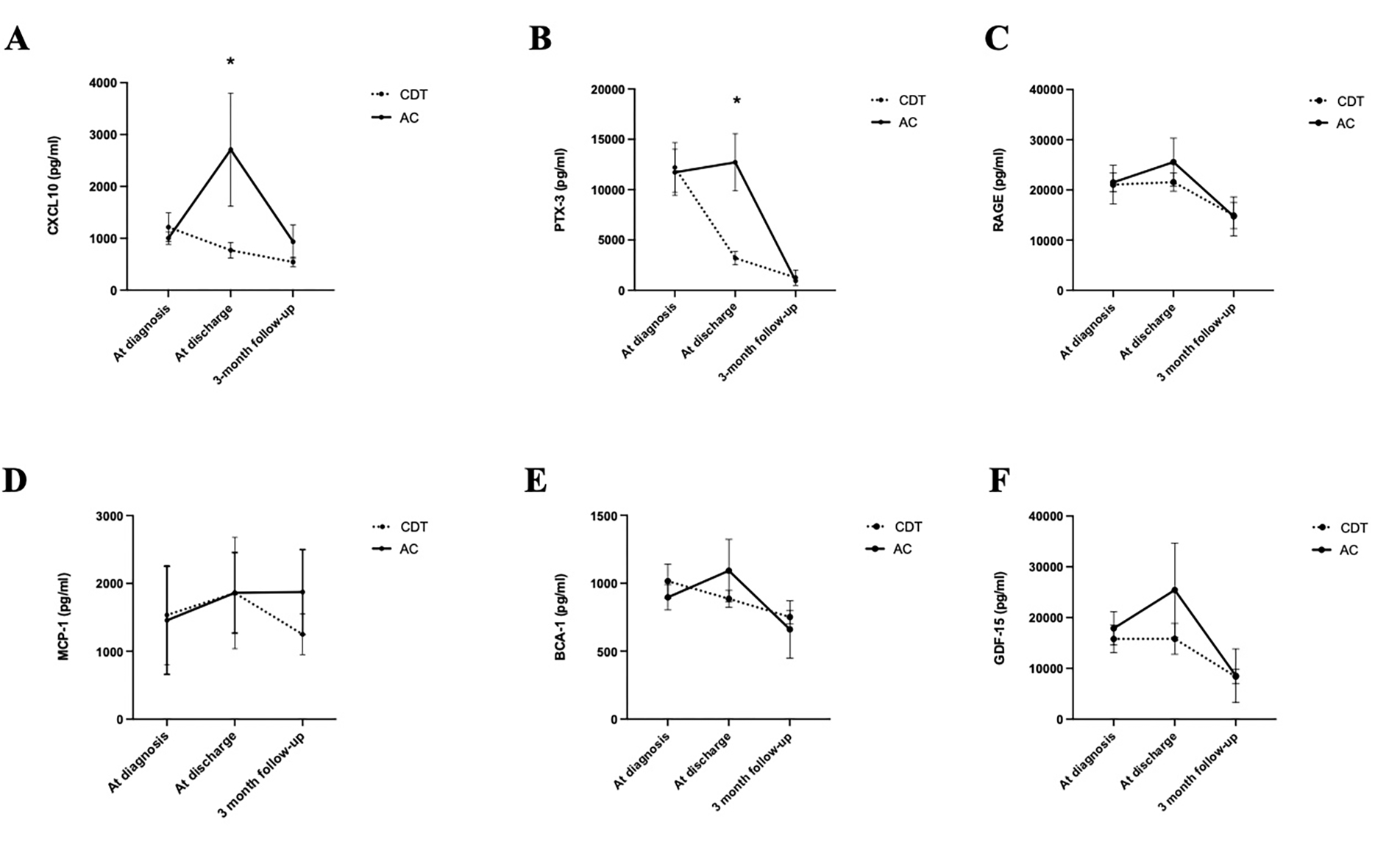
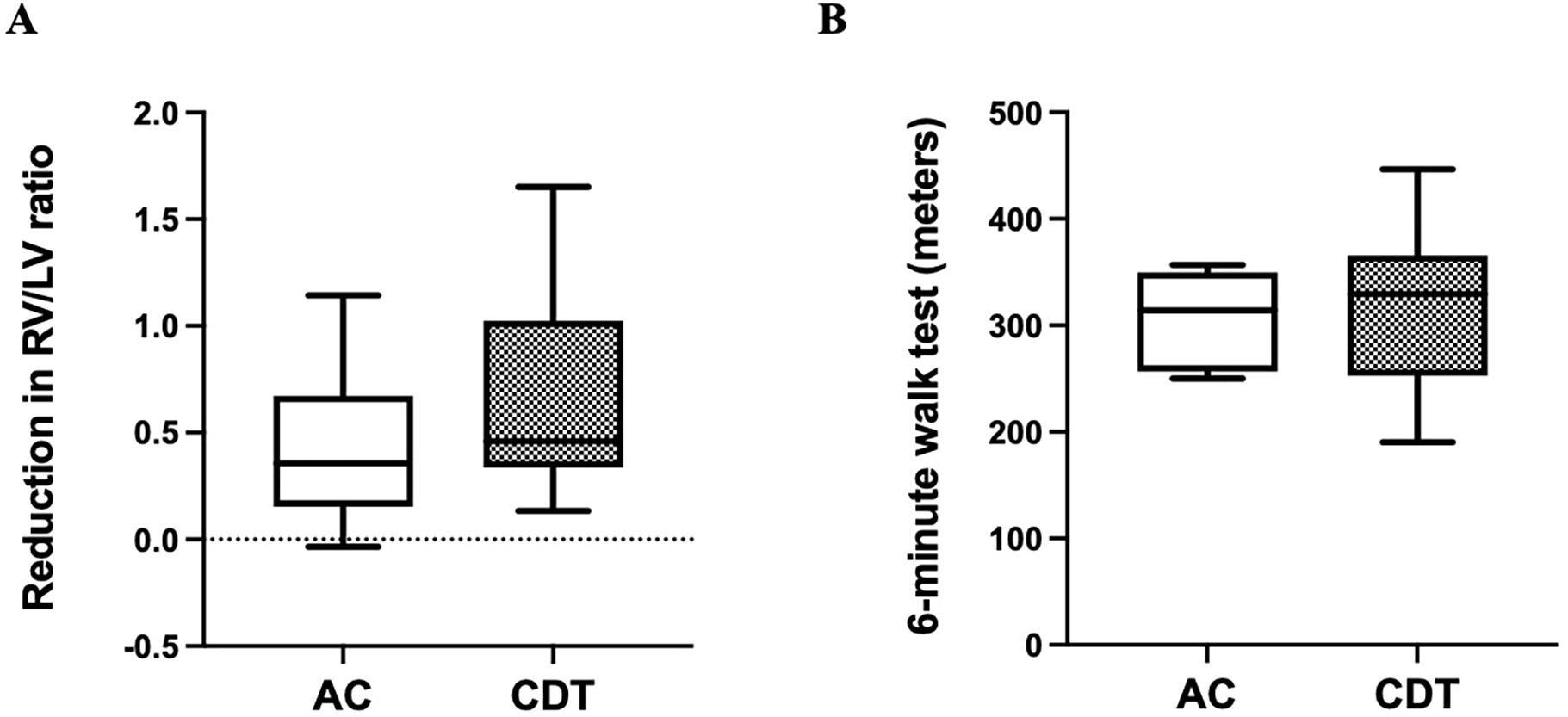
Results: A total of 72 patients (age, 56 ± 15 years; 40.3% women) were included in the present analysis. Of these 72 patients, 53 underwent CDT and 19 were included in the ACA arm. The baseline right ventricle/left ventricle ratios were similar between the two groups (CST, 1.8; ACA, 1.7). The survival and complication rates were similar between the two groups. At discharge, CXCL10 (768.9 ± 148.6 pg/mL vs 3032.0 ± 1201.0 pg/mL; P = .018) and PTX3 (3203.5 ± 1298.0 pg/mL vs 12,716.2 ± 6961.5 pg/mL; P = .029) were lower in the CDT group and displayed a quicker return to baseline than in the ACA group. This trend, although not significant, was also seen with the other biomarkers. At 3 months, the 6-minute walking distance and quality-of-life scores were similar between both groups.
Conclusions: In patients with sPE, the biomarkers of CTEPH were lower with CDT compared with ACA. At 3 months, both groups demonstrated similar biomarker levels, 6-minute walking distances, and quality-of-life scores.
Trial registration: ClinicalTrials.gov NCT02758574.
Keywords: Biomarkers; Catheter-directed thrombolysis; Chronic thromboembolic pulmonary hypertension; Pulmonary embolism.
Copyright © 2023 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
