

Desmopressin for patients with spontaneous intracerebral haemorrhage taking antiplatelet drugs (DASH): a UK-based, phase 2, randomised, placebo-controlled, multicentre feasibility trial
- PMID: 37353276
- PMCID: PMC10284719
- DOI: 10.1016/S1474-4422(23)00157-6
Desmopressin for patients with spontaneous intracerebral haemorrhage taking antiplatelet drugs (DASH): a UK-based, phase 2, randomised, placebo-controlled, multicentre feasibility trial
Abstract
Background: The risk of death from spontaneous intracerebral haemorrhage is increased for people taking antiplatelet drugs. We aimed to assess the feasibility of randomising patients on antiplatelet drug therapy with spontaneous intracerebral haemorrhage to desmopressin or placebo to reduce the antiplatelet drug effect.
Methods: DASH was a phase 2, randomised, placebo-controlled, multicentre feasibility trial. Patients were recruited from ten acute stroke centres in the UK and were eligible if they had an intracerebral haemorrhage with stroke symptom onset within 24 h of randomisation, were aged 18 years or older, and were taking an antiplatelet drug. Participants were randomly assigned (1:1) to a single dose of intravenous desmopressin 20 μg or matching placebo. Treatment allocation was concealed from all staff and patients involved in the trial. The primary outcome was feasibility, which was measured as the number of eligible patients randomised and the proportion of eligible patients approached, and analysis was by intention to treat. The trial was prospectively registered with ISRCTN (reference ISRCTN67038373), and it is closed to recruitment.
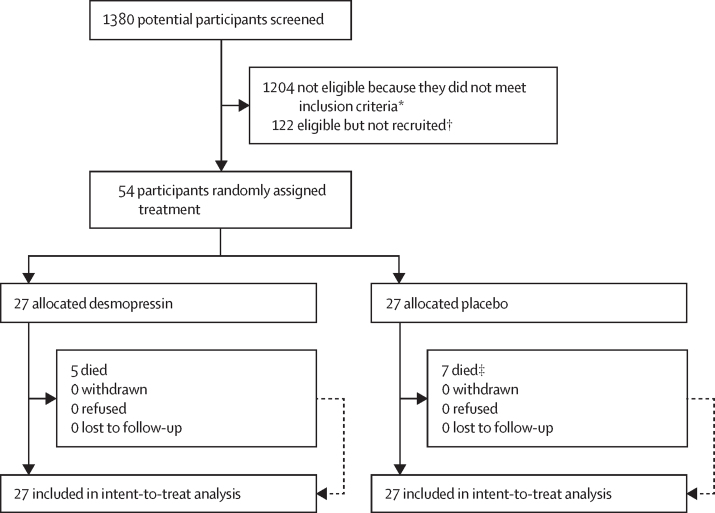
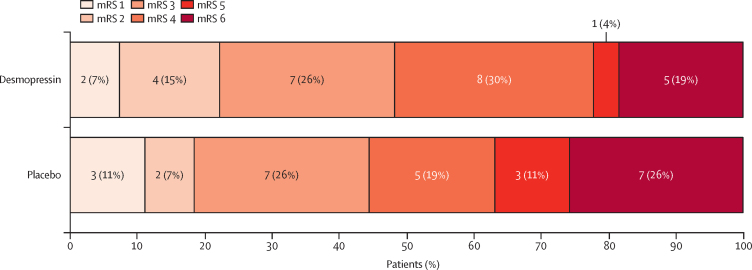
Findings: Between April 1, 2019, and March 31, 2022, 1380 potential participants were screened for eligibility. 176 (13%) participants were potentially eligible, of whom 57 (32%) were approached, and 54 (31%) consented and were subsequently recruited and randomly assigned to receive desmopressin (n=27) or placebo (n=27). The main reason for eligible patients not being recruited was the patient arriving out of hours (74 [61%] of 122 participants). The recruitment rate increased after the enrolment period was extended from 12 h to 24 h, but it was then impaired due to the COVID-19 pandemic. Of the 54 participants included in the analysis (mean age 76·4 years [SD 11·3]), most were male (36 [67%]) and White (50 [93%]). 53 (98%) of 54 participants received all of their allocated treatment (one participant assigned desmopressin only received part of the infusion). No participants were lost to follow-up or withdrew from the trial. Death or dependency on others for daily activities at day 90 (modified Rankin Scale score >4) occurred in six (22%) of 27 participants in the desmopressin group and ten (37%) of 27 participants in the placebo group. Serious adverse events occurred in 12 (44%) participants in the desmopressin group and 13 (48%) participants in the placebo group. The most common adverse events were expansion of the haemorrhagic stroke (four [15%] of 27 participants in the desmopressin group and six [22%] of 27 participants in the placebo group) and pneumonia (one [4%] of 27 participants in the desmopressin group and six [22%] of 27 participants in the placebo group).
Interpretation: Our results show it is feasible to randomise patients with spontaneous intracerebral haemorrhage who are taking antiplatelet drugs to desmopressin or placebo. Our findings support the need for a definitive trial to determine if desmopressin improves outcomes in patients with intracerebral haemorrhage on antiplatelet drug therapy.
Funding: National Institute for Health Research.
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
Comment in
-
Trials in intracerebral haemorrhage: a path to success?Lancet Neurol. 2023 Jul;22(7):542-543. doi: 10.1016/S1474-4422(23)00201-6. Lancet Neurol. 2023. PMID: 37353268 No abstract available.
References
-
- Royal College of Physicians Sentinel Stroke National Audit Programme (SSNAP) 2016. https://www.strokeaudit.org/Documents/National/AcuteOrg/2016/2016-AOANat...
-
- Krishnamurthi RV, Ikeda T, Feigin VL. Global, regional and country-specific burden of ischaemic stroke, intracerebral haemorrhage and subarachnoid haemorrhage: a systematic analysis of the Global Burden of Disease Study 2017. Neuroepidemiology. 2020;54:171–179. - PubMed
-
- Anderson CS, Heeley E, Huang Y, et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. N Engl J Med. 2013;368:2355–2365. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
