

Impact of community-based interventions on out-of-hospital cardiac arrest outcomes: a systematic review and meta-analysis
- PMID: 37353542
- PMCID: PMC10290111
- DOI: 10.1038/s41598-023-35735-y
Impact of community-based interventions on out-of-hospital cardiac arrest outcomes: a systematic review and meta-analysis
Abstract
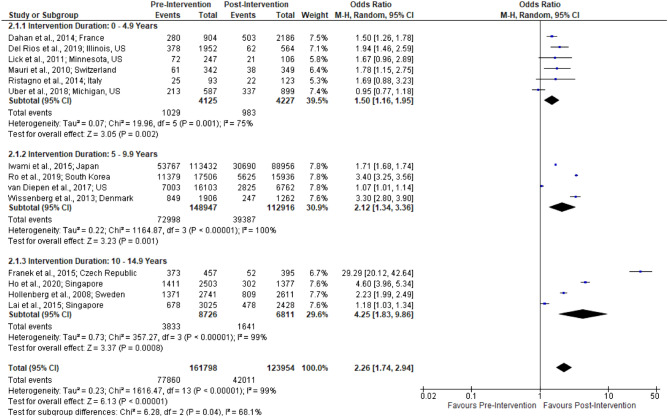
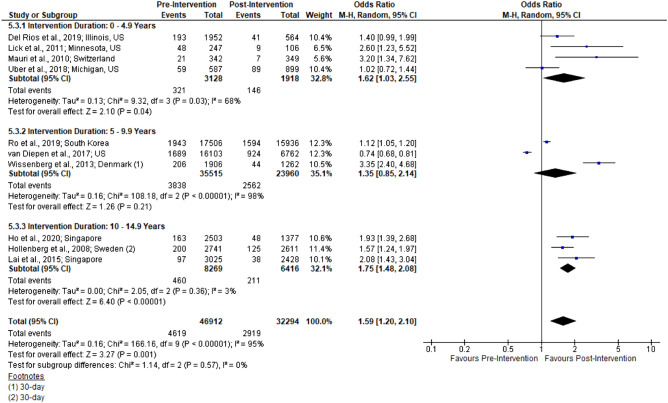
Survival following out-of-hospital cardiac arrest (OHCA) remains low, typically less than 10%. Bystander cardiopulmonary resuscitation (CPR) and bystander-AED use have been shown to improve survival by up to fourfold in individual studies. Numerous community-based interventions have been implemented worldwide in an effort to enhance rates of bystander-CPR, bystander-AED use, and improve OHCA survival. This systematic review and meta-analysis aims to evaluate the effect of such interventions on OHCA outcomes. Medline and Embase were systematically searched from inception through July 2021 for studies describing the implementation and effect of one or more community-based interventions targeting OHCA outcomes. Two reviewers screened articles, extracted data, and evaluated study quality using the Newcastle-Ottawa Scale. For each outcome, data were pooled using random-effects meta-analysis. Of the 2481 studies identified, 16 met inclusion criteria. All included studies were observational. They reported a total of 1,081,040 OHCAs across 11 countries. The most common interventions included community-based CPR training (n = 12), community-based AED training (n = 9), and dispatcher-assisted CPR (n = 8). Health system interventions (hospital or paramedical services) were also described in 11 of the included studies. Evidence certainty among all outcomes was low or very low according to GRADE criteria. On meta-analysis, community-based interventions with and without health system interventions were consistently associated with improved OCHA outcomes: rates of bystander-CPR, bystander-AED use, survival, and survival with a favorable neurological outcome. Bystander CPR-14 studies showed a significant increase in post-intervention bystander-CPR rates (n = 285 752; OR 2.26 [1.74, 2.94]; I2 = 99%, and bystander AED use (n = 37 882; OR 2.08 [1.44, 3.01]; I2 = 54%) and durvival-10 studies, pooling survival to hospital discharge and survival to 30 days (n = 79 206; OR 1.59 [1.20, 2.10]; I2 = 95%. The results provide foundational support for the efficacy of community-based interventions in enhancing OHCA outcomes. These findings inform our recommendation that communities, regions, and countries should implement community-based interventions in their pre-hospital strategy for OHCA. Further research is needed to identify which specific intervention types are most effective.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Graham RMAM, Andrea MS. Strategies to Improve Cardiac Arrest Survival. National Academies Press; 2015. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
