

Emergency medical services utilisation among febrile children attending emergency departments across Europe: an observational multicentre study
- PMID: 37354239
- PMCID: PMC10570223
- DOI: 10.1007/s00431-023-05056-3
Emergency medical services utilisation among febrile children attending emergency departments across Europe: an observational multicentre study
Abstract
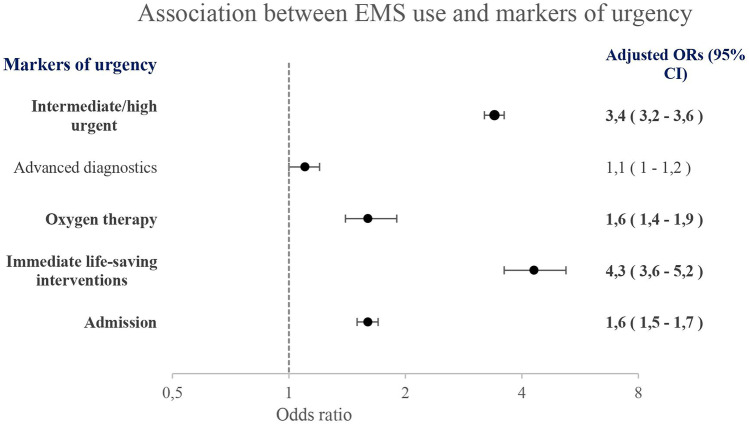
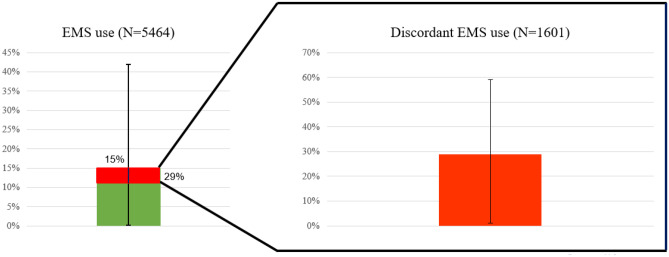
Children constitute 6-10% of all patients attending the emergency department (ED) by emergency medical services (EMS). However, discordant EMS use in children occurs in 37-61% with fever as an important risk factor. We aimed to describe EMS utilisation among febrile children attending European EDs. This study is part of an observational multicentre study assessing management and outcome in febrile children up to 18 years (MOFICHE) attending twelve EDs in eight European countries. Discordant EMS use was defined as the absence of markers of urgency including intermediate/high triage urgency, advanced diagnostics, treatment, and admission in children transferred by EMS. Multivariable logistic regression analyses were performed for the association between (1) EMS use and markers of urgency, and (2) patient characteristics and discordant EMS use after adjusting all analyses for the covariates age, gender, visiting hours, presenting symptoms, and ED setting. A total of 5464 (15%, range 0.1-42%) children attended the ED by EMS. Markers of urgency were more frequently present in the EMS group compared with the non-EMS group. Discordant EMS use occurred in 1601 children (29%, range 1-59%). Age and gender were not associated with discordant EMS use, whereas neurological symptoms were associated with less discordant EMS use (aOR 0.2, 95%CI 0.1-0.2), and attendance out of office hours was associated with more discordant EMS use (aOR 1.6, 95%CI 1.4-1.9). Settings with higher percentage of self-referrals to the ED had more discordant EMS use (p < 0.05). Conclusion: There is large practice variation in EMS use in febrile children attending European EDs. Markers of urgency were more frequently present in children in the EMS group. However, discordant EMS use occurred in 29%. Further research is needed on non-medical factors influencing discordant EMS use in febrile children across Europe, so that pre-emptive strategies can be implemented. What is Known: •Children constitute around 6-10% of all patients attending the emergency department by emergency medical services. •Discordant EMS use occurs in 37-61% of all children, with fever as most common presenting symptom for discordant EMS use in children. What is New: •There is large practice variation in EMS use among febrile children across Europe with discordance EMS use occurring in 29% (range 1-59%), which was associated with attendance during out of office hours and with settings with higher percentage of self-referrals to the ED. •Future research is needed focusing on non-medical factors (socioeconomic status, parental preferences and past experience, healthcare systems, referral pathways, out of hours services provision) that influence discordant EMS use in febrile children across Europe.
Keywords: Children; Emergency care; Emergency medical services; Fever; Paediatrics.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- NHTSA. WHAT IS EMS? : National Highway Traffic Safety AdministrationOffice of Emergency Medical Services; [Available from: https://www.ems.gov/whatisems.html
-
- Ramenofsky ML, Luterman A, Curreri PW, Talley MA (1983) EMS for pediatrics: optimum treatment of unnecessary delay? J Pediatr Surg 18(4):498–504 - PubMed
-
- Tsai AKG. Epidemiology of pediatric prehospital care. 1987;16(3):284–292. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
